S-ar putea să vă placă și
- B16B EngineDocument30 paginiB16B EngineStormÎncă nu există evaluări
- Group 6Document10 paginiGroup 6LINDOHÎncă nu există evaluări
- Section 7 Electrical SystemDocument3 paginiSection 7 Electrical Systemmohamed omerÎncă nu există evaluări
- Hyundai R130W-3 Electrical SystemDocument49 paginiHyundai R130W-3 Electrical SystemHai VanÎncă nu există evaluări
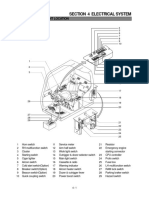
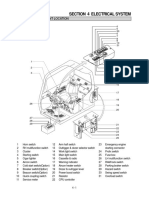
- Section 4 Electrical System: Group 1 Component LocationDocument2 paginiSection 4 Electrical System: Group 1 Component LocationHanh LeÎncă nu există evaluări
- HL-740 (TM) 6-4Document22 paginiHL-740 (TM) 6-4REMZONAÎncă nu există evaluări
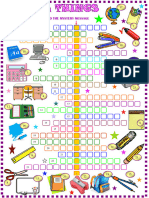
- School Things - Crossword Puzzle With KeyDocument3 paginiSchool Things - Crossword Puzzle With KeyIren ShuflinÎncă nu există evaluări
- Section 7 Electrical System: Group 1 Component LocationDocument2 paginiSection 7 Electrical System: Group 1 Component LocationAlfredo Guzmán100% (1)
- GSC X GXBank Popcorn Run 2023 E-GuidebookDocument16 paginiGSC X GXBank Popcorn Run 2023 E-Guidebookpheiphei.taiÎncă nu există evaluări
- Cardiac Glycosides: 1. General Characteristic 2. Medicinal Plants and Plant Material Containing Cardiac GlycosidesDocument43 paginiCardiac Glycosides: 1. General Characteristic 2. Medicinal Plants and Plant Material Containing Cardiac GlycosidesasaÎncă nu există evaluări
- Libro 1Document10 paginiLibro 1Meliza HuancaÎncă nu există evaluări
- Christmas 3Document2 paginiChristmas 3Yersultan GalymovÎncă nu există evaluări
- 910J618F1 Hoist 1st ReductionDocument2 pagini910J618F1 Hoist 1st ReductionFrancisco Javier González LópezÎncă nu există evaluări
- School Things CrosswordDocument3 paginiSchool Things CrosswordElisabeth gomesÎncă nu există evaluări
- T de Los ManguitosDocument1 paginăT de Los ManguitosppmateuÎncă nu există evaluări
- Aau2 Cutouts U1 PDFDocument1 paginăAau2 Cutouts U1 PDF341389.Încă nu există evaluări
- Group 10 Steering ValveDocument2 paginiGroup 10 Steering Valveعمروصالح كليسÎncă nu există evaluări
- Hélicoptére - Paper Model - Model Kartonowy - Vasyliev Roman (Kampfflieger) - Avro 671 Rota MK 1 PDFDocument3 paginiHélicoptére - Paper Model - Model Kartonowy - Vasyliev Roman (Kampfflieger) - Avro 671 Rota MK 1 PDFMassiMilianoMonteBelloÎncă nu există evaluări
- Section 6 Electrical SystemDocument3 paginiSection 6 Electrical SystemSaidi JalelÎncă nu există evaluări
- Engine No.: 6642331Document1 paginăEngine No.: 6642331geronimojuarez179Încă nu există evaluări
- SUBMERSIBLE PANELS-Model4Document1 paginăSUBMERSIBLE PANELS-Model4ahmed fathyÎncă nu există evaluări
- 3rd DimensionDocument1 pagină3rd DimensionPiancó Câmara MunicipalÎncă nu există evaluări
- BX 32ND3Document2 paginiBX 32ND3Jack HawkeÎncă nu există evaluări
- Sirius-PJ2 (X6181N / WX6181N / WU6181N)Document9 paginiSirius-PJ2 (X6181N / WX6181N / WU6181N)William LozadaÎncă nu există evaluări
- Instructions Ec120bDocument2 paginiInstructions Ec120bAlejandro MamaniÎncă nu există evaluări
- Section 4 Electrical SystemDocument3 paginiSection 4 Electrical SystemDavidÎncă nu există evaluări
- Section 4 Electrical System: Group 1 Component LocationDocument2 paginiSection 4 Electrical System: Group 1 Component LocationBartłomiej StępieńÎncă nu există evaluări
- Schematic Banco de Prueba de Helice 2023-05-05Document1 paginăSchematic Banco de Prueba de Helice 2023-05-05elkakon13Încă nu există evaluări
- Globe ValvesDocument16 paginiGlobe ValvesafazazissaÎncă nu există evaluări
- Lola LC88 GP 88Document5 paginiLola LC88 GP 88Vyktor SousaÎncă nu există evaluări
- Section 4 Electrical System: Group 1 Component LocationDocument2 paginiSection 4 Electrical System: Group 1 Component LocationSONÎncă nu există evaluări
- Canalta Dual Chamber Fitting Exploded View of Internal PartsDocument1 paginăCanalta Dual Chamber Fitting Exploded View of Internal Partsmfg_serviciosÎncă nu există evaluări
- 8FG D CE048-09 - 0608 P SteeringDocument21 pagini8FG D CE048-09 - 0608 P SteeringDuong Van HoanÎncă nu există evaluări
- b20d Frame & BodyDocument84 paginib20d Frame & BodyErick BothaÎncă nu există evaluări
- SCR System Issue 1Document24 paginiSCR System Issue 1Teddy KhantÎncă nu există evaluări
- Resourcesmediakey &language Code En&type DocumentDocument8 paginiResourcesmediakey &language Code En&type DocumentdarkoÎncă nu există evaluări
- MDA NotesDocument12 paginiMDA NotesKISHORE K 20MIY0004Încă nu există evaluări
- Hyundai 130w 3 ElectricalDocument4 paginiHyundai 130w 3 Electricalmary100% (63)
- HL 750 7-1Document2 paginiHL 750 7-1REMZONA100% (1)
- Control Valve 4 Spool 2 8Document2 paginiControl Valve 4 Spool 2 8eshopmanual TigaÎncă nu există evaluări
- WDR IFtDocument3 paginiWDR IFtMetehan KaraÎncă nu există evaluări
- Food, Drinks and Groceries CrosswordsDocument3 paginiFood, Drinks and Groceries CrosswordsPaola NoriegaÎncă nu există evaluări
- ZSC PILOT Reg Partes de RepuestoDocument4 paginiZSC PILOT Reg Partes de RepuestoJuan JuanÎncă nu există evaluări
- Denah Kamar Operasi Rsud LembangDocument1 paginăDenah Kamar Operasi Rsud LembangariÎncă nu există evaluări
- 6-1 Component LocationDocument3 pagini6-1 Component LocationkrisnaÎncă nu există evaluări
- Main Rev1 Circuit 2Document1 paginăMain Rev1 Circuit 2Relu IanoviciÎncă nu există evaluări
- BLADIMIRDocument16 paginiBLADIMIRHernan Eliseo BairesÎncă nu există evaluări
- Section 4 Electrical System: Group 1 Component LocationDocument2 paginiSection 4 Electrical System: Group 1 Component LocationTaha RdmanÎncă nu există evaluări
- Starmill Smartstep Electrical DrawingsDocument29 paginiStarmill Smartstep Electrical Drawingsgad lunaÎncă nu există evaluări
- Group 4 Disassembly and Assembly: 1. Brake PumpDocument6 paginiGroup 4 Disassembly and Assembly: 1. Brake PumpTaha RdmanÎncă nu există evaluări
- D100118334 - 1 - Glass Fiber - 136X561X1685MM - SF - MF and LF Cabins - 1Document1 paginăD100118334 - 1 - Glass Fiber - 136X561X1685MM - SF - MF and LF Cabins - 1Louis Rivera CasoÎncă nu există evaluări
- Food and Drinks CrosswordDocument3 paginiFood and Drinks CrosswordFaiber IbarraÎncă nu există evaluări
- Critical Path MethodDocument1 paginăCritical Path MethodSheena FarinasÎncă nu există evaluări
- ESCAPEDocument1 paginăESCAPEEmilio CortesÎncă nu există evaluări
- Group 10 Steering ValveDocument2 paginiGroup 10 Steering ValveTaha RdmanÎncă nu există evaluări
- Type Z Pilot Regulators: Parts ListDocument4 paginiType Z Pilot Regulators: Parts ListCentro De Belleza Rizos EstiloÎncă nu există evaluări
- Parts List RA750 / RA850: Hydraulic / Electrical SchematicsDocument79 paginiParts List RA750 / RA850: Hydraulic / Electrical SchematicsFenix MechanicsÎncă nu există evaluări
- 00 Manual de Partes REIMERDocument79 pagini00 Manual de Partes REIMERFenix MechanicsÎncă nu există evaluări
- Despiece Hyosung Aquila GV 125Document119 paginiDespiece Hyosung Aquila GV 125Oriel Merino CortesÎncă nu există evaluări
- The Power of Scarcity: Leveraging Urgency and Demand to Influence Customer DecisionsDe la EverandThe Power of Scarcity: Leveraging Urgency and Demand to Influence Customer DecisionsÎncă nu există evaluări
- Preload and AfterloadDocument28 paginiPreload and Afterloadapi-19916399100% (1)
- Physiology - Retired QuestionsDocument12 paginiPhysiology - Retired Questionsapi-19916399Încă nu există evaluări
- Respiration 3Document23 paginiRespiration 3api-19916399100% (1)
- Blood CoagulationDocument70 paginiBlood Coagulationapi-19916399Încă nu există evaluări
- Respiration TwoDocument58 paginiRespiration Twoapi-19916399Încă nu există evaluări
- Physiology Answers and ExDocument19 paginiPhysiology Answers and Exapi-19916399Încă nu există evaluări
- Nervous System 7Document20 paginiNervous System 7api-19916399Încă nu există evaluări
- Jingying T.A. Department of PhysiologyDocument22 paginiJingying T.A. Department of Physiologyapi-19916399Încă nu există evaluări
- Nervous System 6Document27 paginiNervous System 6api-19916399Încă nu există evaluări
- Physiology of Blood VesselDocument65 paginiPhysiology of Blood Vesselapi-19916399Încă nu există evaluări
- Jingying T.A. Department of PhysiologyDocument19 paginiJingying T.A. Department of Physiologyapi-19916399Încă nu există evaluări
- Neurophysiology: Run Fight Speak Think Watch Listen Taste SmellDocument22 paginiNeurophysiology: Run Fight Speak Think Watch Listen Taste Smellapi-19916399Încă nu există evaluări
- Jingying T.A. Department of PhysiologyDocument26 paginiJingying T.A. Department of Physiologyapi-19916399Încă nu există evaluări
- Electrophysiological Properties of Cardiac MyocytesDocument39 paginiElectrophysiological Properties of Cardiac Myocytesapi-19916399Încă nu există evaluări
- Kyuhyun Wang, MD: What Is The Rhythm?Document43 paginiKyuhyun Wang, MD: What Is The Rhythm?api-19916399Încă nu există evaluări
- 01.introduction To PhysiologyDocument44 pagini01.introduction To Physiologyapi-19916399Încă nu există evaluări
- Evaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac IndexDocument53 paginiEvaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac Indexapi-19916399Încă nu există evaluări
- Circulation4 5Document1 paginăCirculation4 5api-19916399Încă nu există evaluări
- Gastrointestinal PhysiologDocument133 paginiGastrointestinal Physiologapi-19916399100% (1)
- Gastrointestinal PhysiologyDocument134 paginiGastrointestinal Physiologyapi-19916399100% (1)
- Electrical Activity of The HeartDocument29 paginiElectrical Activity of The Heartapi-19916399Încă nu există evaluări
- Evaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac IndexDocument53 paginiEvaluation of Pumping Function of Heart: Stroke Volume Cardiac Output Ejection Fraction Cardiac Indexapi-19916399Încă nu există evaluări
- Rhythmical Excitation of The HeartDocument29 paginiRhythmical Excitation of The Heartapi-19916399Încă nu există evaluări
- Chapter 2 - 1 - ForeignerDocument35 paginiChapter 2 - 1 - Foreignerapi-19916399Încă nu există evaluări
- Physiology of Blood VesselDocument65 paginiPhysiology of Blood Vesselapi-19916399Încă nu există evaluări
- Chapter Blood: RBC Platelet HemostasisDocument89 paginiChapter Blood: RBC Platelet Hemostasisapi-19916399100% (1)
- AMC Online - Recalls - V3Document167 paginiAMC Online - Recalls - V3Halfida100% (3)
- WSC Questions Answer KeyDocument4 paginiWSC Questions Answer KeyNaimish TripathiÎncă nu există evaluări
- CH 073 Shock in Office PracticeDocument8 paginiCH 073 Shock in Office PracticeLaxmikant RathiÎncă nu există evaluări
- PGI PEDS Emergency Medicine IICDocument351 paginiPGI PEDS Emergency Medicine IICMuthu V RanÎncă nu există evaluări
- Complete Pediatrics (455-512) 1Document58 paginiComplete Pediatrics (455-512) 1Nimesh Kumara100% (2)
- 2 - Anatomy of Salivary Glands EditedDocument18 pagini2 - Anatomy of Salivary Glands EditedHenok BelyaÎncă nu există evaluări
- Important Causes of Sudden Cardiac DeathDocument2 paginiImportant Causes of Sudden Cardiac DeathTausif AbbasÎncă nu există evaluări
- Rheumatology NotesDocument10 paginiRheumatology NotesBrandonRyanF.MosidinÎncă nu există evaluări
- KeratitisDocument16 paginiKeratitisHarmin AliminÎncă nu există evaluări
- Hydatid Disease (Hydatidosis)Document17 paginiHydatid Disease (Hydatidosis)Office EPHÎncă nu există evaluări
- Reg Rujukan Eksternal 26 Juni-25 Juli 2021Document54 paginiReg Rujukan Eksternal 26 Juni-25 Juli 2021RuciÎncă nu există evaluări
- Course Task Unit 3Document2 paginiCourse Task Unit 3BSN 1-YA-22 ELITIONG, MARY JEAN A.Încă nu există evaluări
- Instructions For Use of MedicinesDocument195 paginiInstructions For Use of MedicinesOleg SoyaÎncă nu există evaluări
- Stress Breeding-Disease ResistanceDocument6 paginiStress Breeding-Disease ResistanceYASHPAL SINGHÎncă nu există evaluări
- Parasitology Notes - SLU Lictag FrancesDocument49 paginiParasitology Notes - SLU Lictag FrancesJmarc JubiladoÎncă nu există evaluări
- Detection of Inva Gene of Salmonella From Milkfish (Chanos Chanos) at Sidoarjo Wet Fish Market, Indonesia, Using Polymerase Chain Reaction TechniqueDocument7 paginiDetection of Inva Gene of Salmonella From Milkfish (Chanos Chanos) at Sidoarjo Wet Fish Market, Indonesia, Using Polymerase Chain Reaction TechniqueMarsha NajlaÎncă nu există evaluări
- Laboratory Exercise No. 02 1Document7 paginiLaboratory Exercise No. 02 1Christian Grajo GualvezÎncă nu există evaluări
- Health and Illness British English Teacher Ver2Document4 paginiHealth and Illness British English Teacher Ver2Marta ПартутаÎncă nu există evaluări
- Case Fatality RateDocument7 paginiCase Fatality RateMuhammad salman alfayedÎncă nu există evaluări
- Heat Stroke: This Photo by Unknown Author Is Licensed UnderDocument10 paginiHeat Stroke: This Photo by Unknown Author Is Licensed UnderMinakshi MawariÎncă nu există evaluări
- Varicose VeinsDocument8 paginiVaricose VeinshalesÎncă nu există evaluări
- Ent MCQ 22-23 For StudentsDocument46 paginiEnt MCQ 22-23 For StudentsBharathi Sneha PeriasamyÎncă nu există evaluări
- 3 GENPATHO To Be PrintDocument25 pagini3 GENPATHO To Be PrintDENTAL REVIEWER ONLYÎncă nu există evaluări
- Paragraf Pandemic Disease Coronavirus Disease (Covid-19) : Diajukan Guna Memenuhi Tugas Mata Kuliah Bahasa InggrisDocument3 paginiParagraf Pandemic Disease Coronavirus Disease (Covid-19) : Diajukan Guna Memenuhi Tugas Mata Kuliah Bahasa InggrisJulfianasÎncă nu există evaluări
- 1-Kelley's Cancer Therapy - This Is The Cure For CancerDocument11 pagini1-Kelley's Cancer Therapy - This Is The Cure For CancerSusyary S100% (2)
- 11 Types of Headaches - Causes, Symptoms, and TreatmentDocument27 pagini11 Types of Headaches - Causes, Symptoms, and TreatmentCHIMA ONWUKA MONGÎncă nu există evaluări
- Macrocytosis - What Causes It - Mayo ClinicDocument3 paginiMacrocytosis - What Causes It - Mayo ClinicvmarinelliÎncă nu există evaluări
- 3 - Summary & MCQs PDFDocument6 pagini3 - Summary & MCQs PDFSrinivas PingaliÎncă nu există evaluări
- Who Can Perform Arterial Blood Collection?Document4 paginiWho Can Perform Arterial Blood Collection?Yna BurgosÎncă nu există evaluări
- Science Olympiad Anatomy & Physiology 2014Document2 paginiScience Olympiad Anatomy & Physiology 2014Alicia Hyland82% (11)