S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Diabetes Dengan Xanthoma KulitDocument2 paginiDiabetes Dengan Xanthoma KulitNovriefta NugrahaÎncă nu există evaluări
- Embryology&TeratologyDocument43 paginiEmbryology&TeratologyNovriefta NugrahaÎncă nu există evaluări
- Islamic MedicineDocument16 paginiIslamic MedicineNovriefta NugrahaÎncă nu există evaluări
- Journal of XanthomaDocument5 paginiJournal of XanthomaNovriefta NugrahaÎncă nu există evaluări
- Tugas Journal ReadingDocument34 paginiTugas Journal ReadingNovriefta NugrahaÎncă nu există evaluări
- Pediatrics 2004 Garcia Peña 24 8Document7 paginiPediatrics 2004 Garcia Peña 24 8Novriefta NugrahaÎncă nu există evaluări
- Dengue Guideline DengueDocument33 paginiDengue Guideline DenguedrkkdbÎncă nu există evaluări
- Newcastle OttawaDocument3 paginiNewcastle OttawaNovriefta NugrahaÎncă nu există evaluări
- 05 Nose AnatomyDocument28 pagini05 Nose AnatomyNovriefta NugrahaÎncă nu există evaluări
- Results of Case-Control Studies Support Association Between Contact Lens Use andDocument17 paginiResults of Case-Control Studies Support Association Between Contact Lens Use andNovriefta NugrahaÎncă nu există evaluări
- Respiratory EmergenciesDocument30 paginiRespiratory EmergenciesNovriefta NugrahaÎncă nu există evaluări
- Journal of Ultrasonography in Acute AppendisitisDocument7 paginiJournal of Ultrasonography in Acute AppendisitisNovriefta NugrahaÎncă nu există evaluări
- COPD, Asthma, and DM Risk FactorDocument13 paginiCOPD, Asthma, and DM Risk FactorNovriefta NugrahaÎncă nu există evaluări
- Ankle Brachial Pressure IndexDocument12 paginiAnkle Brachial Pressure IndexNovriefta NugrahaÎncă nu există evaluări
- ARITMIA, Gangguan Irama JantungDocument37 paginiARITMIA, Gangguan Irama JantungNovriefta NugrahaÎncă nu există evaluări
- Handbook of Pathology and Pathophysiology of Cardiovascular Disease 2002 PDFDocument321 paginiHandbook of Pathology and Pathophysiology of Cardiovascular Disease 2002 PDFChavo Delocho100% (1)
- WHO - Surgical Care at The District Hospital (WHO 2003)Document514 paginiWHO - Surgical Care at The District Hospital (WHO 2003)gekriaÎncă nu există evaluări
- Terminology of The Tonsils: 2011 Blackwell Verlag GMBH - Anat. Histol. Embryol. 40 (2011) 204-209Document7 paginiTerminology of The Tonsils: 2011 Blackwell Verlag GMBH - Anat. Histol. Embryol. 40 (2011) 204-209Novriefta NugrahaÎncă nu există evaluări
- 05 Nose AnatomyDocument28 pagini05 Nose AnatomyNovriefta NugrahaÎncă nu există evaluări
- Atypical Bacteria in Adenoids and Tonsils of Children Requiring AdenotonsillectomyDocument7 paginiAtypical Bacteria in Adenoids and Tonsils of Children Requiring AdenotonsillectomyNovriefta NugrahaÎncă nu există evaluări
- Allergic Rhinitis 2Document4 paginiAllergic Rhinitis 2Novriefta NugrahaÎncă nu există evaluări
- 05 Nose AnatomyDocument28 pagini05 Nose AnatomyNovriefta NugrahaÎncă nu există evaluări
- Vertigo PeriferDocument76 paginiVertigo PeriferAstriana IndrawatiÎncă nu există evaluări
- UPLOAD KE-1 HormDocument47 paginiUPLOAD KE-1 HormNovriefta NugrahaÎncă nu există evaluări
- Photo Quiz: Enlarged Tonsils and FatigueDocument3 paginiPhoto Quiz: Enlarged Tonsils and FatigueNovriefta NugrahaÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Plant Based Plan White PaperDocument24 paginiPlant Based Plan White PaperSara AdemovicÎncă nu există evaluări
- Bellows and Expansion JointsDocument5 paginiBellows and Expansion JointsSuresh MechÎncă nu există evaluări
- Artifact 7 - Superannuation Pension Calculator-GuidelinesDocument2 paginiArtifact 7 - Superannuation Pension Calculator-GuidelinesSai RamÎncă nu există evaluări
- Healing and Keeping Prayer (2013)Document2 paginiHealing and Keeping Prayer (2013)Kylie DanielsÎncă nu există evaluări
- 1101259L 580.752830 Pressure Washer ManualDocument64 pagini1101259L 580.752830 Pressure Washer Manualgork1roguesÎncă nu există evaluări
- Herbs and SpicesDocument77 paginiHerbs and SpicesNicole RicohermosoÎncă nu există evaluări
- Vocabulary June v22Document2 paginiVocabulary June v22Wiston TonwisÎncă nu există evaluări
- Cocktail Making Techniques 13.3.11Document3 paginiCocktail Making Techniques 13.3.11Ryan MenezesÎncă nu există evaluări
- Jokes and Their Relation To The Unconscious: Laurence HenkelmanDocument3 paginiJokes and Their Relation To The Unconscious: Laurence HenkelmanMilos VisnjicÎncă nu există evaluări
- Chinese Cinderella - MeDocument2 paginiChinese Cinderella - Meapi-298120057100% (1)
- Argumentative EssayDocument5 paginiArgumentative EssayJoshua MontoyaÎncă nu există evaluări
- Weaning Guidelines 2007Document4 paginiWeaning Guidelines 2007deliejoyceÎncă nu există evaluări
- Clinical Algorithms in General Surgery PDFDocument786 paginiClinical Algorithms in General Surgery PDFLaura Campaña100% (5)
- POFL Unit 1 Status QUO pp.1-37Document38 paginiPOFL Unit 1 Status QUO pp.1-37AruÎncă nu există evaluări
- Kmartinez Draft Research PaperDocument14 paginiKmartinez Draft Research Paperapi-273007806Încă nu există evaluări
- English 10-1 Personal Response EssayDocument2 paginiEnglish 10-1 Personal Response Essayapi-467840192Încă nu există evaluări
- ISKCON Desire Tree - Brahma Vimohana LeelaDocument34 paginiISKCON Desire Tree - Brahma Vimohana LeelaISKCON desire treeÎncă nu există evaluări
- Main Group Oganometallics: Shriver and Atkins, Chapter 15Document24 paginiMain Group Oganometallics: Shriver and Atkins, Chapter 15José Augusto VillarÎncă nu există evaluări
- Expository Cause and Effect OUTLINEDocument2 paginiExpository Cause and Effect OUTLINEAutoDefenceÎncă nu există evaluări
- 8-Critical Appraisal of An ArticleDocument20 pagini8-Critical Appraisal of An ArticleMohmmed Abu MahadyÎncă nu există evaluări
- Pipe Thickness CalculationDocument4 paginiPipe Thickness CalculationHarryÎncă nu există evaluări
- DICGC - For Depositors - A Guide To Deposit InsuranceDocument10 paginiDICGC - For Depositors - A Guide To Deposit InsuranceSachinÎncă nu există evaluări
- Major Head of AccountsDocument9 paginiMajor Head of AccountsArun EmmiÎncă nu există evaluări
- Vice President Quality Operations in Greater Chicago IL Resume Kevin FredrichDocument2 paginiVice President Quality Operations in Greater Chicago IL Resume Kevin FredrichKevin Fredrich1Încă nu există evaluări
- Enzymes in Grain ProcessingDocument1 paginăEnzymes in Grain ProcessingAttila-Levente FogarasiÎncă nu există evaluări
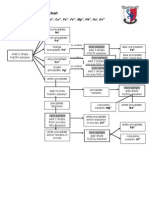
- Testing For Cations Flow ChartDocument2 paginiTesting For Cations Flow Chartapi-252561013Încă nu există evaluări
- EVK203/EVK213/EVK223/EVK233/EVK253: Digital Thermostats For Ventilated Refrigerating UnitsDocument2 paginiEVK203/EVK213/EVK223/EVK233/EVK253: Digital Thermostats For Ventilated Refrigerating UnitsMihai BordeianuÎncă nu există evaluări
- 9 SolutionsDocument31 pagini9 SolutionsLaurertan TavaresÎncă nu există evaluări
- Polycystic Ovary Syndrome (PCOS) - Symptoms, Causes, and TreatmentDocument19 paginiPolycystic Ovary Syndrome (PCOS) - Symptoms, Causes, and TreatmentAkshay HarekarÎncă nu există evaluări
- Modelling The Effects of Condensate Banking On High CGR ReservoirsDocument11 paginiModelling The Effects of Condensate Banking On High CGR ReservoirslikpataÎncă nu există evaluări