S-ar putea să vă placă și
- Lecture 2-Blood RBC WBCDocument51 paginiLecture 2-Blood RBC WBCsamayaÎncă nu există evaluări
- The Circulatory System: BloodDocument59 paginiThe Circulatory System: BloodKristian Dave DivaÎncă nu există evaluări
- Anatomy and Physiology of BLOOD: Preet KaurDocument37 paginiAnatomy and Physiology of BLOOD: Preet KaurPreet KaurÎncă nu există evaluări
- BloodDocument80 paginiBloodHem Chandra ShahÎncă nu există evaluări
- BloodDocument76 paginiBloodKerby Dela Fuente Alison100% (1)
- CVS BloodDocument39 paginiCVS BloodMohan GuptaÎncă nu există evaluări
- BloodDocument49 paginiBloodDale TelgenhoffÎncă nu există evaluări
- Case 11Document63 paginiCase 11حكيم العجلانÎncă nu există evaluări
- The Circulatory System: BloodDocument69 paginiThe Circulatory System: BloodMozesCuateÎncă nu există evaluări
- BLOOD LecDocument46 paginiBLOOD LecGrape JuiceÎncă nu există evaluări
- AnaemiasDocument60 paginiAnaemiasbvkjtzrvnyÎncă nu există evaluări
- 1 BloodDocument77 pagini1 BloodVisaNathan100% (1)
- BLOOD Update-1Document56 paginiBLOOD Update-1ahmadfadi343Încă nu există evaluări
- Blood Cells, Immunity and Blood ClottingDocument65 paginiBlood Cells, Immunity and Blood Clottingmunaamuummee100% (1)
- Blood: Cardiovascular SystemDocument75 paginiBlood: Cardiovascular SystemTina MinottÎncă nu există evaluări
- Haemopoiesis: Composition of Whole Blood & Its ComponentsDocument8 paginiHaemopoiesis: Composition of Whole Blood & Its ComponentsSafiya JamesÎncă nu există evaluări
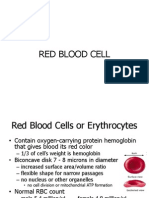
- Topics of This Lecture: RBC: - Structural Characteristics - Hemoglobin - Erythropoiesis - Erythrocytes DestructionDocument23 paginiTopics of This Lecture: RBC: - Structural Characteristics - Hemoglobin - Erythropoiesis - Erythrocytes DestructionHashim GhazoÎncă nu există evaluări
- Hematologic DisordersDocument30 paginiHematologic DisordersUday Kumar100% (1)
- PSG 712 Blood-1Document54 paginiPSG 712 Blood-1preciousÎncă nu există evaluări
- Hematology 2020Document63 paginiHematology 2020odiodi57Încă nu există evaluări
- Body Fluids and Their Circulation 1Document96 paginiBody Fluids and Their Circulation 1sanmathiÎncă nu există evaluări
- Blood: - Hematopoiesis (Hemopoiesis) : Blood CellDocument5 paginiBlood: - Hematopoiesis (Hemopoiesis) : Blood Cellflay1618Încă nu există evaluări
- Physiology of Blood: Ratna Kusumawati Department of Physiology, Faculty of Medicine Universitas Sebelas Maret SurakartaDocument60 paginiPhysiology of Blood: Ratna Kusumawati Department of Physiology, Faculty of Medicine Universitas Sebelas Maret SurakartaZidaneÎncă nu există evaluări
- Physiology of Blood: Ratna Kusumawati Department of Physiology, Faculty of Medicine Universitas Sebelas Maret SurakartaDocument65 paginiPhysiology of Blood: Ratna Kusumawati Department of Physiology, Faculty of Medicine Universitas Sebelas Maret SurakartaRizal AbdurrahmanÎncă nu există evaluări
- Functions of BloodDocument12 paginiFunctions of BloodAngieRamirezÎncă nu există evaluări
- Blood: - The Only Fluid Tissue in The Human Body - Classified As A Connective TissueDocument39 paginiBlood: - The Only Fluid Tissue in The Human Body - Classified As A Connective TissueJorÎncă nu există evaluări
- 1-Blood Composition and FunctionDocument43 pagini1-Blood Composition and FunctionKaleem Mohammad100% (2)
- Blood: - Enzymes, E.G. Certain Clotting FactorsDocument14 paginiBlood: - Enzymes, E.G. Certain Clotting FactorsDerrick kinyaÎncă nu există evaluări
- Introduction To HematologyDocument95 paginiIntroduction To HematologyAhmad Farhan Hassan0% (1)
- Chapter 4 Blood Coagulation and Coagulation DisordersDocument27 paginiChapter 4 Blood Coagulation and Coagulation DisordersdaisysintszwaiÎncă nu există evaluări
- Red Blood Cells, Anemia, and PolycythemiaDocument7 paginiRed Blood Cells, Anemia, and PolycythemiaShi no Me100% (1)
- LEC3Document26 paginiLEC3Jessica StewartÎncă nu există evaluări
- Blood: Group 1Document25 paginiBlood: Group 1Arian May MarcosÎncă nu există evaluări
- Biology Part-1 NotesDocument59 paginiBiology Part-1 NotesgjbxÎncă nu există evaluări
- Physio. D. Suroor. L1. BloodDocument24 paginiPhysio. D. Suroor. L1. Bloodزين العابدين محمد عويشÎncă nu există evaluări
- RBC DISORDERS Part I VR 2022Document63 paginiRBC DISORDERS Part I VR 2022victoria tavasÎncă nu există evaluări
- Module 9 - 4 - Circulatory SystemDocument34 paginiModule 9 - 4 - Circulatory SystemThea Shaine B. SILARDEÎncă nu există evaluări
- Fisiologi Cairan Tubuh & Darah: Dr. Nindya Aryanty, M.Med - EdDocument43 paginiFisiologi Cairan Tubuh & Darah: Dr. Nindya Aryanty, M.Med - EdIman TaufiqÎncă nu există evaluări
- Blood Lecture PowerpointDocument116 paginiBlood Lecture Powerpointdrmarybeth100% (3)
- Nurs 107 Blood Physiology Lecture 4Document46 paginiNurs 107 Blood Physiology Lecture 4Ann AgyeiwaaÎncă nu există evaluări
- Blood PDFDocument55 paginiBlood PDFlorrainebarandonÎncă nu există evaluări
- PHS 221 1Document44 paginiPHS 221 1metasynthronos748Încă nu există evaluări
- Hematopoiesis and ErytherokiniticsDocument20 paginiHematopoiesis and ErytherokiniticsShahid F.S.D.Încă nu există evaluări
- Blood Physiology-Lecture 4Document54 paginiBlood Physiology-Lecture 4alfaristurkiÎncă nu există evaluări
- Introd., Haemopoiesis & Plasma ProteinsDocument119 paginiIntrod., Haemopoiesis & Plasma ProteinsShamsuddeen UsmanÎncă nu există evaluări
- 6.2 Human BloodDocument48 pagini6.2 Human BloodSmart ThemisÎncă nu există evaluări
- Blood PhysiologyDocument8 paginiBlood PhysiologypjcaneroÎncă nu există evaluări
- Blood and Blood ComponentsDocument19 paginiBlood and Blood ComponentsMiljun CatacataÎncă nu există evaluări
- University of Guyana Health Sciences FacultyDocument44 paginiUniversity of Guyana Health Sciences FacultySatrohan SurjnarineÎncă nu există evaluări
- Lecture 9 CVSDocument118 paginiLecture 9 CVSMuhammad Abbas WaliÎncă nu există evaluări
- Cardiovascular Physiology 4Document75 paginiCardiovascular Physiology 4maxmus4Încă nu există evaluări
- Haemopoetic SystemDocument73 paginiHaemopoetic SystemManjunathÎncă nu există evaluări
- Blood Lectures 2014 PIO 205Document84 paginiBlood Lectures 2014 PIO 205Philip Abayomi VincentÎncă nu există evaluări
- Ch18 BloodDocument31 paginiCh18 BloodNoah DominoÎncă nu există evaluări
- RBC DISORDERS StudentsDocument84 paginiRBC DISORDERS Studentskimberly abianÎncă nu există evaluări
- Avian Physiology Lecture 003Document36 paginiAvian Physiology Lecture 003Susai Mari NixonÎncă nu există evaluări
- Blood Part 1Document35 paginiBlood Part 1Keziah TampusÎncă nu există evaluări
- Red Blood Cells, Functions, Diseases A Simple Guide To The Condition, Diagnosis, Treatment, And Related ConditionsDe la EverandRed Blood Cells, Functions, Diseases A Simple Guide To The Condition, Diagnosis, Treatment, And Related ConditionsÎncă nu există evaluări
- Fast Facts: Deficiencia de piruvato quinasa para pacientes y familiares: Una enfermedad genética rara que afecta a los glóbulos rojos Información + Asumir el control = El mejor resultadoDe la EverandFast Facts: Deficiencia de piruvato quinasa para pacientes y familiares: Una enfermedad genética rara que afecta a los glóbulos rojos Información + Asumir el control = El mejor resultadoÎncă nu există evaluări
- Without This Message by Purchasing Novapdf : Print To PDFDocument1 paginăWithout This Message by Purchasing Novapdf : Print To PDFvanderphysÎncă nu există evaluări
- 9 Skeletal SystemDocument63 pagini9 Skeletal Systemvanderphys100% (1)
- Study of Microscopic Anatomy - Only 200 Different Cells Types - Four Primary Tissue ClassesDocument61 paginiStudy of Microscopic Anatomy - Only 200 Different Cells Types - Four Primary Tissue ClassesvanderphysÎncă nu există evaluări
- Cells Capable of Shortening & Converting The Chemical Energy of ATP Into Mechanical Energy - Types of Muscle - Physiology of Skeletal MuscleDocument64 paginiCells Capable of Shortening & Converting The Chemical Energy of ATP Into Mechanical Energy - Types of Muscle - Physiology of Skeletal MusclevanderphysÎncă nu există evaluări
- 16 Sense OrgansDocument79 pagini16 Sense OrgansvanderphysÎncă nu există evaluări
- Nucleus and Nucleic Acids - Protein Synthesis and Secretion - DNA Replication and The Cell Cycle - Chromosomes and HeredityDocument53 paginiNucleus and Nucleic Acids - Protein Synthesis and Secretion - DNA Replication and The Cell Cycle - Chromosomes and HeredityvanderphysÎncă nu există evaluări
- Study of Microscopic Anatomy - Only 200 Different Cells Types - Four Primary Tissue ClassesDocument61 paginiStudy of Microscopic Anatomy - Only 200 Different Cells Types - Four Primary Tissue ClassesvanderphysÎncă nu există evaluări
- 600 Human Skeletal Muscles - General Structural & Functional OrganizationDocument61 pagini600 Human Skeletal Muscles - General Structural & Functional OrganizationvanderphysÎncă nu există evaluări
- 14 The Central Nervous SystemDocument61 pagini14 The Central Nervous SystemvanderphysÎncă nu există evaluări
- 8 Bone TissueDocument39 pagini8 Bone Tissuevanderphys100% (1)
- 25 Digestive SystemDocument79 pagini25 Digestive SystemvanderphysÎncă nu există evaluări
- 7 Integumentary SystemDocument38 pagini7 Integumentary Systemvanderphys100% (1)
- 22 Respiratory SystemDocument99 pagini22 Respiratory SystemvanderphysÎncă nu există evaluări
- 25 Digestive SystemDocument79 pagini25 Digestive SystemvanderphysÎncă nu există evaluări
- Evaluation of Global Research Trends in The Area of Food Waste D - 2020 - Food CDocument10 paginiEvaluation of Global Research Trends in The Area of Food Waste D - 2020 - Food CAliÎncă nu există evaluări
- 300.91C - Fire Alarm System Pre-Test and Acceptance Test Checklist 3-27-14Document2 pagini300.91C - Fire Alarm System Pre-Test and Acceptance Test Checklist 3-27-14mthuyaÎncă nu există evaluări
- Philips Family Lamp UV CDocument4 paginiPhilips Family Lamp UV CmaterpcÎncă nu există evaluări
- Ar ExportsDocument1 paginăAr ExportsRais AlamÎncă nu există evaluări
- Tsang Mui Millennium School 2019-2020 English Worksheet: Fill in The Blanks With The Correct Form of The VerbsDocument46 paginiTsang Mui Millennium School 2019-2020 English Worksheet: Fill in The Blanks With The Correct Form of The VerbscocoyipÎncă nu există evaluări
- MicrosoftDynamicsNAVAdd OnsDocument620 paginiMicrosoftDynamicsNAVAdd OnsSadiq QudduseÎncă nu există evaluări
- Watercolor SecretsDocument60 paginiWatercolor Secretsmissdoisneau98% (47)
- Hydrostatic, Deviatoric StressesDocument7 paginiHydrostatic, Deviatoric StressespanbuÎncă nu există evaluări
- DuctBank For Electrical SystemDocument4 paginiDuctBank For Electrical SystemAnonymous XYAPaxjbYÎncă nu există evaluări
- Chapter 1 Cumulative Review: Multiple ChoiceDocument2 paginiChapter 1 Cumulative Review: Multiple ChoiceJ. LeeÎncă nu există evaluări
- Moving Money Box: Pig (Assembly Instructions) : The Movements Work Better With Heavier CoinsDocument6 paginiMoving Money Box: Pig (Assembly Instructions) : The Movements Work Better With Heavier CoinsjuanÎncă nu există evaluări
- 19 Free Amigurumi Crochet Patterns: MaterialsDocument4 pagini19 Free Amigurumi Crochet Patterns: MaterialsLucica Diaconu100% (1)
- Long Quiz 1 Eim Tools, MaterialsDocument1 paginăLong Quiz 1 Eim Tools, MaterialsLea Ann PalaciosÎncă nu există evaluări
- Beauty Therapy Thesis SampleDocument8 paginiBeauty Therapy Thesis Samplerachelvalenzuelaglendale100% (2)
- TSBDocument3 paginiTSBnoe dela vegaÎncă nu există evaluări
- Oc818 Manual v03-1Document5 paginiOc818 Manual v03-1Luca PayetÎncă nu există evaluări
- Cooking Off The Clock by Elizabeth Falkner - Recipes and ExcerptDocument16 paginiCooking Off The Clock by Elizabeth Falkner - Recipes and ExcerptThe Recipe ClubÎncă nu există evaluări
- Saberon StratMan2Document3 paginiSaberon StratMan2paredesladyheart18Încă nu există evaluări
- UNDP NP Dhangadhi SWM TOR FinalDocument4 paginiUNDP NP Dhangadhi SWM TOR FinalNirmal K.c.Încă nu există evaluări
- Air Cooler With Checking DoorDocument2 paginiAir Cooler With Checking DoorSuraj KumarÎncă nu există evaluări
- Toda People in IndiaDocument9 paginiToda People in IndiaAmoona KopiKoÎncă nu există evaluări
- (Q2) Electrochemistry 29th JulyDocument21 pagini(Q2) Electrochemistry 29th JulySupritam KunduÎncă nu există evaluări
- NMMT City Bus SystemDocument3 paginiNMMT City Bus Systemharish guptaÎncă nu există evaluări
- Lesson 2 Arts of East AsiaDocument21 paginiLesson 2 Arts of East Asiarenaldo ocampoÎncă nu există evaluări
- Unit Test 7 (PDF)Document1 paginăUnit Test 7 (PDF)emirelliucÎncă nu există evaluări
- De Thi Vao 10 Chuyen Hoa Nguyen Trai Hai Duong 20212022Document2 paginiDe Thi Vao 10 Chuyen Hoa Nguyen Trai Hai Duong 20212022Trần Ngọc BíchÎncă nu există evaluări
- Sunday Afternoon, October 27, 2013: TechnologyDocument283 paginiSunday Afternoon, October 27, 2013: TechnologyNatasha MyersÎncă nu există evaluări
- Carriages and Mounts SeriesDocument92 paginiCarriages and Mounts Seriessudhirm16Încă nu există evaluări
- Iec TR 62343-6-8-2011Document14 paginiIec TR 62343-6-8-2011Amer AmeryÎncă nu există evaluări
- Vision For Mobile Robot Navigation - A Survey PDFDocument31 paginiVision For Mobile Robot Navigation - A Survey PDFtes donlodÎncă nu există evaluări