S-ar putea să vă placă și
- Seborrheic Dermatitis Overview AafpDocument6 paginiSeborrheic Dermatitis Overview Aafpcaptaincandy11Încă nu există evaluări
- PEPTIC ULCER: CAUSES, SYMPTOMS AND TREATMENTDocument18 paginiPEPTIC ULCER: CAUSES, SYMPTOMS AND TREATMENTIrfandy Chairi Sulaiman LubisÎncă nu există evaluări
- Baca BTKV - DR Suhardi - 28-8-2014Document17 paginiBaca BTKV - DR Suhardi - 28-8-2014Rizky FachriÎncă nu există evaluări
- Bimbingan TtsDocument7 paginiBimbingan TtsRizky FachriÎncă nu există evaluări
- Daftar Penyakit Kemampuan 4Document9 paginiDaftar Penyakit Kemampuan 4Rizky FachriÎncă nu există evaluări
- Bimbingan TtsDocument7 paginiBimbingan TtsRizky FachriÎncă nu există evaluări
- Jurnal Reading ApengDocument23 paginiJurnal Reading ApengRizky FachriÎncă nu există evaluări
- Rekap Pasien Bedah Digestive Baru 1Document11 paginiRekap Pasien Bedah Digestive Baru 1Andri MuliaÎncă nu există evaluări
- Hipertensi PBLDocument56 paginiHipertensi PBLVandra PrinosaÎncă nu există evaluări
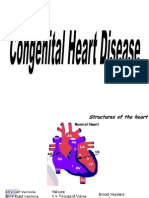
- Congenital Heart DiseaseDocument58 paginiCongenital Heart DiseaseAndre Dreyva ErniÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Efolio 404Document7 paginiEfolio 404api-377789171Încă nu există evaluări
- Op-Ed ObesityDocument3 paginiOp-Ed Obesityapi-302568521Încă nu există evaluări
- Epifeed LHFDocument2 paginiEpifeed LHFJoko WiwiÎncă nu există evaluări
- Safety Policy PDFDocument2 paginiSafety Policy PDFAnonymous Y6VYmM7zÎncă nu există evaluări
- Medicinal Benefits of Minor MilletsDocument4 paginiMedicinal Benefits of Minor MilletsIJARBS JOURNALÎncă nu există evaluări
- MEDSURG - Cellular AberrationDocument10 paginiMEDSURG - Cellular AberrationLeslie CruzÎncă nu există evaluări
- 1.1. What Is Stress?: Chapter Six-Stress ManagementDocument6 pagini1.1. What Is Stress?: Chapter Six-Stress ManagementMikias DegwaleÎncă nu există evaluări
- Tumor StagingDocument9 paginiTumor Stagingmalaran.deboraheloisaÎncă nu există evaluări
- Diagnosis of PregnancyDocument26 paginiDiagnosis of PregnancyMounikaÎncă nu există evaluări
- FPTP - Amoxicillin - Clavulanic Acid in Cats With & Without Chronic Kidney DiseaseDocument2 paginiFPTP - Amoxicillin - Clavulanic Acid in Cats With & Without Chronic Kidney DiseaseMabe AguirreÎncă nu există evaluări
- Public Availability of Labeling CBE Guidance PDFDocument6 paginiPublic Availability of Labeling CBE Guidance PDFMichael wangÎncă nu există evaluări
- Traffic Rules LiteracyDocument11 paginiTraffic Rules LiteracyMaricel AycoÎncă nu există evaluări
- Back From The Bluez - 09 - Self ManagementDocument5 paginiBack From The Bluez - 09 - Self ManagementMelanie DovaleÎncă nu există evaluări
- Differential Diagnosis of Cervicobrachial PainDocument11 paginiDifferential Diagnosis of Cervicobrachial PainpuchioÎncă nu există evaluări
- Local Honey Might Help Your AllergiesDocument3 paginiLocal Honey Might Help Your AllergiesDaniel JadeÎncă nu există evaluări
- Malignant Struma OvariiDocument4 paginiMalignant Struma Ovariixwahyu 108Încă nu există evaluări
- Cecilia Laurente Theory of Nursing Practice and CareDocument1 paginăCecilia Laurente Theory of Nursing Practice and CareChandria Chandria100% (1)
- AEFIDocument33 paginiAEFIAnuradha JaiswalÎncă nu există evaluări
- Ecoglobal Foundation - Jean-Philippe HenryDocument22 paginiEcoglobal Foundation - Jean-Philippe HenryEnergy for AllÎncă nu există evaluări
- CV FormatDocument1 paginăCV FormatpanchodomÎncă nu există evaluări
- Philippines Volume 10 FernDocument2 paginiPhilippines Volume 10 FernJen Aquino ZetaÎncă nu există evaluări
- TonsillitisDocument21 paginiTonsillitisWael ShamyÎncă nu există evaluări
- ACLS Megacode Checklist For StudentsDocument3 paginiACLS Megacode Checklist For StudentsKhrisha Anne DavilloÎncă nu există evaluări
- Marjory GordonDocument7 paginiMarjory GordonPusimah IsmayfiÎncă nu există evaluări
- Social Marketing in Public HealthDocument23 paginiSocial Marketing in Public HealthNurab MartinsÎncă nu există evaluări
- Life Esidimeni Fact SheetDocument4 paginiLife Esidimeni Fact SheetPrimedia Broadcasting100% (2)
- BP FluorideTherapyDocument4 paginiBP FluorideTherapyKavana SrinivasÎncă nu există evaluări
- Alter, Klein - 2008 - The Hazards of Blood Transfusion in Historical PerspectiveDocument11 paginiAlter, Klein - 2008 - The Hazards of Blood Transfusion in Historical Perspectivesushmakumari009Încă nu există evaluări
- Package Pricing at Mission Hospital IMB527 PDFDocument9 paginiPackage Pricing at Mission Hospital IMB527 PDFMasooma SheikhÎncă nu există evaluări
- First Aid and Water SurvivalDocument18 paginiFirst Aid and Water Survivalmusubi purpleÎncă nu există evaluări