S-ar putea să vă placă și
- 08.blueprints Surgery 5th EdDocument70 pagini08.blueprints Surgery 5th EdFadi AlkhassawnehÎncă nu există evaluări
- Diagnostic Features of Disease: Based on French's Index of Differential DiagnosisDe la EverandDiagnostic Features of Disease: Based on French's Index of Differential DiagnosisEvaluare: 1 din 5 stele1/5 (1)
- Duodenal Stump LeakageDocument14 paginiDuodenal Stump LeakageCosmin NicolescuÎncă nu există evaluări
- Pouchitis and Ileal Pouch Disorders: A Multidisciplinary Approach for Diagnosis and ManagementDe la EverandPouchitis and Ileal Pouch Disorders: A Multidisciplinary Approach for Diagnosis and ManagementÎncă nu există evaluări
- ABSITE CH 25 ThoracicDocument11 paginiABSITE CH 25 ThoracicJames JosephÎncă nu există evaluări
- Urinary System: Cytology, Histology, Cystoscopy, and RadiologyDe la EverandUrinary System: Cytology, Histology, Cystoscopy, and RadiologyÎncă nu există evaluări
- Absite CH 32 BilliaryDocument14 paginiAbsite CH 32 BilliaryJames JosephÎncă nu există evaluări
- Liquid Biopsy in Urogenital Cancers and its Clinical UtilityDe la EverandLiquid Biopsy in Urogenital Cancers and its Clinical UtilitySeyed Mohammad Kazem AghamirÎncă nu există evaluări
- ABSITE CH 10 Nutrition PDFDocument8 paginiABSITE CH 10 Nutrition PDFJames JosephÎncă nu există evaluări
- The Guide to Breast Reconstruction: Step-By-Step from Mastectomy Through ReconstructionDe la EverandThe Guide to Breast Reconstruction: Step-By-Step from Mastectomy Through ReconstructionEvaluare: 4 din 5 stele4/5 (1)
- Abdominal Surgery All in OneDocument50 paginiAbdominal Surgery All in OneAnne ChoyÎncă nu există evaluări
- Rectal Cancer PPT 2.1Document131 paginiRectal Cancer PPT 2.1Usmle GuyÎncă nu există evaluări
- Surgery ManualDocument444 paginiSurgery Manualnoor hishamÎncă nu există evaluări
- Oral Boards 2Document67 paginiOral Boards 2Steven GodelmanÎncă nu există evaluări
- Urogenital TumorDocument71 paginiUrogenital TumorJanet UngÎncă nu există evaluări
- SURGERY Lecture 1 - Small Intestine (Dr. Mendoza)Document16 paginiSURGERY Lecture 1 - Small Intestine (Dr. Mendoza)Medisina101100% (1)
- Absite Review QuestionsDocument81 paginiAbsite Review QuestionsJames JosephÎncă nu există evaluări
- Surgery UpcamDocument11 paginiSurgery UpcamArchie DuqueÎncă nu există evaluări
- Fat EmbolismDocument26 paginiFat Embolismdrkadiyala2Încă nu există evaluări
- Gall Stone Disease: DR M.farhad General SurgeonDocument56 paginiGall Stone Disease: DR M.farhad General SurgeondrelvÎncă nu există evaluări
- Carcinoma Penis Management: Dr. Lilamani Rajthala MS Resident Moderator: Dr. Samir ShresthaDocument63 paginiCarcinoma Penis Management: Dr. Lilamani Rajthala MS Resident Moderator: Dr. Samir ShresthaBibek GhimireÎncă nu există evaluări
- Vascular Injury (Prof. Paul, PIT IKABI XV, 14-16 Juli 05)Document53 paginiVascular Injury (Prof. Paul, PIT IKABI XV, 14-16 Juli 05)Wiwin RahayuÎncă nu există evaluări
- DR - Abeidi's Review FinalDocument157 paginiDR - Abeidi's Review FinalSandra AbboudÎncă nu există evaluări
- PSGS Review 2015Document230 paginiPSGS Review 2015yassercarlomanÎncă nu există evaluări
- General Surgery (Must Know)Document93 paginiGeneral Surgery (Must Know)Binit BharatiÎncă nu există evaluări
- Abdominal Trauma: Supervised By: Dr. Hussein Al-HeisDocument63 paginiAbdominal Trauma: Supervised By: Dr. Hussein Al-HeisRashed ShatnawiÎncă nu există evaluări
- Preparing Severely Jaundiced Patient For SurgeryDocument2 paginiPreparing Severely Jaundiced Patient For Surgerylentini@maltanet.netÎncă nu există evaluări
- Dr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza HospitalDocument83 paginiDr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza Hospitalpt.mahmoudÎncă nu există evaluări
- Chapter 5 ATLSDocument27 paginiChapter 5 ATLSUlfaa MutiaaÎncă nu există evaluări
- Surgery Viva QuestionsDocument16 paginiSurgery Viva QuestionsChris Lam Cui ShanÎncă nu există evaluări
- Schwartz UrologyDocument10 paginiSchwartz UrologyRem Alfelor100% (1)
- PeritonitisDocument34 paginiPeritonitisabrar_zaidiÎncă nu există evaluări
- Screenshot 2023-01-22 at 19.25.23Document49 paginiScreenshot 2023-01-22 at 19.25.23Lika BukhaidzeÎncă nu există evaluări
- Bowel AnastomosisDocument30 paginiBowel AnastomosismrashaiedehÎncă nu există evaluări
- Rectal ProlapseDocument29 paginiRectal ProlapseErick AkwanÎncă nu există evaluări
- Экз. воп для 5-го курса на англ. 200 вопросовDocument32 paginiЭкз. воп для 5-го курса на англ. 200 вопросовKumar AdityaÎncă nu există evaluări
- Cardiovascular MCQsDocument23 paginiCardiovascular MCQssb medexÎncă nu există evaluări
- Bariatric SurgeryDocument26 paginiBariatric SurgeryAmyandÎncă nu există evaluări
- Aetiology, Pathology and Management of Enterocutaneous FistulaDocument34 paginiAetiology, Pathology and Management of Enterocutaneous Fistularoselinekhadija100% (1)
- Surgtest GI Surgery NEET SS 2022 RecallDocument58 paginiSurgtest GI Surgery NEET SS 2022 RecallRajhan 410Încă nu există evaluări
- Fast HugDocument41 paginiFast HugBharti NaraÎncă nu există evaluări
- Systemic Surgery NuggetsDocument17 paginiSystemic Surgery NuggetsAhmad UsmanÎncă nu există evaluări
- Chest Tube and Water-Seal DrainageDocument25 paginiChest Tube and Water-Seal DrainageGhadaÎncă nu există evaluări
- SDK Bowel AnastomosisDocument43 paginiSDK Bowel Anastomosisprabowoaji12100% (1)
- Colorectal Cancer 1Document71 paginiColorectal Cancer 1Anupam SisodiaÎncă nu există evaluări
- Hilar Cholangiocarcinoma: Therapeutic Strategies: MT KhalfallahDocument49 paginiHilar Cholangiocarcinoma: Therapeutic Strategies: MT KhalfallahKhalfallah Mohamed TaharÎncă nu există evaluări
- Diagnosis and Treatment of Intraabdominal InjuriesDocument88 paginiDiagnosis and Treatment of Intraabdominal Injuriessgod34Încă nu există evaluări
- Transhiatal EsophagectomyDocument12 paginiTranshiatal EsophagectomyprofarmahÎncă nu există evaluări
- Bile Duct InjuryDocument62 paginiBile Duct InjuryShashidhara Puttaraj100% (1)
- Final General Surgery (1) - 230122 - 192353Document49 paginiFinal General Surgery (1) - 230122 - 192353Lika BukhaidzeÎncă nu există evaluări
- Thoracic Decortication: Sabita Chalise Bns 3 YearDocument32 paginiThoracic Decortication: Sabita Chalise Bns 3 YearRamchandra Chalise100% (1)
- D2 Gastrectomy: DR K Suneel Kaushik Senior Resident Surgical OncologyDocument66 paginiD2 Gastrectomy: DR K Suneel Kaushik Senior Resident Surgical OncologySuneel Kaushik KÎncă nu există evaluări
- Blunt Adominal TraumaDocument14 paginiBlunt Adominal TraumaMuhammad Bima AkbarÎncă nu există evaluări
- TOACS With KEYDocument25 paginiTOACS With KEYMehwish MughalÎncă nu există evaluări
- In Service Exam For Breast DR Paul BalisiDocument11 paginiIn Service Exam For Breast DR Paul BalisiAmiel Francisco ReyesÎncă nu există evaluări
- Ultimate Surgery MCQDocument104 paginiUltimate Surgery MCQSivakumar Kathuu KarthikeyanÎncă nu există evaluări
- 008 Plain X-Ray AbdomenDocument7 pagini008 Plain X-Ray AbdomenAthul GurudasÎncă nu există evaluări
- Intra Abdominal 2009Document8 paginiIntra Abdominal 2009Shinta Dwi Septiani Putri WibowoÎncă nu există evaluări
- RRM's Next - TraumaDocument284 paginiRRM's Next - TraumaRamkishan NekkantiÎncă nu există evaluări
- MalariaDocument27 paginiMalariabagusÎncă nu există evaluări
- How To Prevent Progressivity DMDocument60 paginiHow To Prevent Progressivity DMbagusÎncă nu există evaluări
- Abdominal Injury KNH GITHAIGA 2Document42 paginiAbdominal Injury KNH GITHAIGA 2bagusÎncă nu există evaluări
- MalariaDocument27 paginiMalariabagusÎncă nu există evaluări
- 5607TNCC-Abdominal TraumaDocument65 pagini5607TNCC-Abdominal Traumabagus100% (1)
- Extrapyramidal System DisordersDocument69 paginiExtrapyramidal System DisordersbagusÎncă nu există evaluări
- Guillain Barré SyndromeDocument21 paginiGuillain Barré SyndromebagusÎncă nu există evaluări
- WHO - Q&as On HypertensionDocument3 paginiWHO - Q&as On HypertensionbagusÎncă nu există evaluări
- 7 Liver - Spleen TraumaDocument34 pagini7 Liver - Spleen Traumabagus75% (4)
- 751 1523 1 PBgukDocument11 pagini751 1523 1 PBgukbagusÎncă nu există evaluări
- How To Be Successful in Job Interview Akper PemprovDocument13 paginiHow To Be Successful in Job Interview Akper PemprovbagusÎncă nu există evaluări
- Rich Text Editor FileDocument1 paginăRich Text Editor FilebagusÎncă nu există evaluări
- 12.7.09 RoseJones GBSDocument15 pagini12.7.09 RoseJones GBSAgnes NesiaÎncă nu există evaluări
- BFNDocument1 paginăBFNbagusÎncă nu există evaluări
- Rich Text Editor FileaeffDocument1 paginăRich Text Editor FileaeffbagusÎncă nu există evaluări
- Preview (1) .Mp3Document1 paginăPreview (1) .Mp3bagusÎncă nu există evaluări
- Basic Management of - Maxillofacial Trauma1Document26 paginiBasic Management of - Maxillofacial Trauma1Pratikshya KothiaÎncă nu există evaluări
- Bls Class CPR Power PointDocument45 paginiBls Class CPR Power Point2020 MSc bhuvaneswari 05100% (1)
- Pediatric CPRDocument18 paginiPediatric CPRNoor A. ZakiÎncă nu există evaluări
- Basic Life Support Ms 2 Rle Term 2 PDFDocument4 paginiBasic Life Support Ms 2 Rle Term 2 PDFJesha PlatigueÎncă nu există evaluări
- Chapter 9 - Thoracic Injuries Questions: Dr. Achmad Faisal, SPBTKV, Fects, FihaDocument12 paginiChapter 9 - Thoracic Injuries Questions: Dr. Achmad Faisal, SPBTKV, Fects, FihaRifka Anisa0% (1)
- Airway-RSI Pocket CardDocument4 paginiAirway-RSI Pocket CardbellerevolteÎncă nu există evaluări
- Ruptur Diafragma WikipediaDocument6 paginiRuptur Diafragma WikipediaAndi Upik FathurÎncă nu există evaluări
- PROJECT PROPOSAL 1st Aid TRNGDocument4 paginiPROJECT PROPOSAL 1st Aid TRNGJOEL DAEN100% (1)
- Triage & TransportDocument28 paginiTriage & TransportiqiqiqiqiqÎncă nu există evaluări
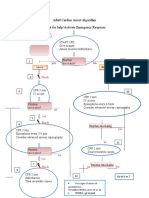
- Adult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseDocument1 paginăAdult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseICU RSBMÎncă nu există evaluări
- Fellowship Personal Statements ExamplesDocument57 paginiFellowship Personal Statements ExamplesFellowship Personal Statements Samples100% (11)
- Thoracic TraumaDocument12 paginiThoracic TraumaNiarti Ulan Sari SiarnuÎncă nu există evaluări
- Ambulance BrochureDocument2 paginiAmbulance Brochureapi-494939117Încă nu există evaluări
- Standard First AidDocument96 paginiStandard First AidahCURSED100% (9)
- Dial 1298 For Ambulance - HSBCDocument22 paginiDial 1298 For Ambulance - HSBCDial1298forAmbulanceÎncă nu există evaluări
- Cover - Panduan - 021 - 036 - RSU Manado Medical CenterDocument99 paginiCover - Panduan - 021 - 036 - RSU Manado Medical CenterAdrian SahayÎncă nu există evaluări
- Basic Ventilator y ModesDocument47 paginiBasic Ventilator y ModesAlina VanceaÎncă nu există evaluări
- Emergency First Aid and CPRDocument15 paginiEmergency First Aid and CPRvhlactaotaoÎncă nu există evaluări
- Epimn Module 1 Triage During A Mass Casualty IncidentDocument48 paginiEpimn Module 1 Triage During A Mass Casualty IncidentZodiac AdamsÎncă nu există evaluări
- Unit 10 Fist AidDocument81 paginiUnit 10 Fist AidillimooniteÎncă nu există evaluări
- NAEMT AMLS CommitteeDocument2 paginiNAEMT AMLS CommitteeJim ThorntonÎncă nu există evaluări
- Set Rec Pic 829Document2 paginiSet Rec Pic 829Peter SalimÎncă nu există evaluări
- Atls PDFDocument34 paginiAtls PDFrchristevenÎncă nu există evaluări
- Carnival Medical Positions DetailsDocument6 paginiCarnival Medical Positions DetailsEliseo CastroÎncă nu există evaluări
- Jason Wolfe's ATLS Trauma Moulage Page: (Thoughts On The Management of The Multiply Injured Patient)Document18 paginiJason Wolfe's ATLS Trauma Moulage Page: (Thoughts On The Management of The Multiply Injured Patient)gogopal100% (6)
- C-Mac Stylet For Et Tube PlacementDocument2 paginiC-Mac Stylet For Et Tube Placementamor kermayaÎncă nu există evaluări
- Jurnal Reading American Heart Association Focused Update On Adult Basic Life Support and Cardiopulmonary Resuscitation QualityDocument17 paginiJurnal Reading American Heart Association Focused Update On Adult Basic Life Support and Cardiopulmonary Resuscitation QualitydinageubrinaÎncă nu există evaluări
- Triage PPT DownloadDocument15 paginiTriage PPT DownloadEmergency ABMCÎncă nu există evaluări
- Do Not Resuscitate Confirmation Form: To Direct The Practice of Paramedics and Firefighters After February 1, 2008Document2 paginiDo Not Resuscitate Confirmation Form: To Direct The Practice of Paramedics and Firefighters After February 1, 2008eschiuÎncă nu există evaluări
- BLSPPT 180126100212 PDFDocument58 paginiBLSPPT 180126100212 PDFAdolfo Sven Gomez MolinaÎncă nu există evaluări
- Peaceful Sleep Hypnosis: Meditate & RelaxDe la EverandPeaceful Sleep Hypnosis: Meditate & RelaxEvaluare: 4.5 din 5 stele4.5/5 (142)
- Breaking the Habit of Being YourselfDe la EverandBreaking the Habit of Being YourselfEvaluare: 4.5 din 5 stele4.5/5 (1458)
- Summary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissDe la EverandSummary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissEvaluare: 4.5 din 5 stele4.5/5 (81)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipDe la EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipEvaluare: 4.5 din 5 stele4.5/5 (1135)
- Gut Health Hacks: 200 Ways to Balance Your Gut Microbiome and Improve Your Health!De la EverandGut Health Hacks: 200 Ways to Balance Your Gut Microbiome and Improve Your Health!Evaluare: 4.5 din 5 stele4.5/5 (20)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDe la EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningEvaluare: 4 din 5 stele4/5 (3)
- Love Yourself, Heal Your Life Workbook (Insight Guide)De la EverandLove Yourself, Heal Your Life Workbook (Insight Guide)Evaluare: 5 din 5 stele5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- Bedtime Stories for Adults: Tales to Soothe the Tired SoulsDe la EverandBedtime Stories for Adults: Tales to Soothe the Tired SoulsEvaluare: 4 din 5 stele4/5 (3)
- Forever Strong: A New, Science-Based Strategy for Aging WellDe la EverandForever Strong: A New, Science-Based Strategy for Aging WellÎncă nu există evaluări
- The Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerDe la EverandThe Happiest Baby on the Block: The New Way to Calm Crying and Help Your Newborn Baby Sleep LongerEvaluare: 4.5 din 5 stele4.5/5 (58)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisDe la EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisEvaluare: 3 din 5 stele3/5 (2)
- Really Very Crunchy: A Beginner's Guide to Removing Toxins from Your Life without Adding Them to Your PersonalityDe la EverandReally Very Crunchy: A Beginner's Guide to Removing Toxins from Your Life without Adding Them to Your PersonalityEvaluare: 5 din 5 stele5/5 (28)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonDe la EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonEvaluare: 3.5 din 5 stele3.5/5 (33)
- Deep Sleep Hypnosis: Fall Asleep Instantly And Sleep WellDe la EverandDeep Sleep Hypnosis: Fall Asleep Instantly And Sleep WellEvaluare: 5 din 5 stele5/5 (8)
- Deep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!De la EverandDeep Sleep Meditation: Fall Asleep Instantly with Powerful Guided Meditations, Hypnosis, and Affirmations. Overcome Anxiety, Depression, Insomnia, Stress, and Relax Your Mind!Evaluare: 4.5 din 5 stele4.5/5 (10)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayDe la EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayÎncă nu există evaluări
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeDe la EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeEvaluare: 3.5 din 5 stele3.5/5 (13)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeDe la EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeÎncă nu există evaluări
- Deep Sleep Hypnosis: Guided Meditation For Sleep & HealingDe la EverandDeep Sleep Hypnosis: Guided Meditation For Sleep & HealingEvaluare: 4.5 din 5 stele4.5/5 (103)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouDe la EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouEvaluare: 3.5 din 5 stele3.5/5 (5)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookDe la EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookEvaluare: 3.5 din 5 stele3.5/5 (2)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingDe la EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingEvaluare: 4 din 5 stele4/5 (3)
- Fast Asleep: Improve Brain Function, Lose Weight, Boost Your Mood, Reduce Stress, and Become a Better SleeperDe la EverandFast Asleep: Improve Brain Function, Lose Weight, Boost Your Mood, Reduce Stress, and Become a Better SleeperEvaluare: 4.5 din 5 stele4.5/5 (15)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyDe la EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyÎncă nu există evaluări