S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- AnxietyDocument48 paginiAnxietyGira HirparaÎncă nu există evaluări
- 1 - Case Disfagia DisfoniaDocument41 pagini1 - Case Disfagia DisfoniaMegan ShanzuÎncă nu există evaluări
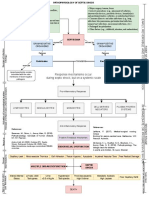
- Pathophysiology of Septic Shock Draft 1Document1 paginăPathophysiology of Septic Shock Draft 1Ju Lie AnnÎncă nu există evaluări
- Pediatrics PG Exam PapersDocument39 paginiPediatrics PG Exam Paperscooldude_secbad1712100% (1)
- Tetracycline HCL Drug StudyDocument4 paginiTetracycline HCL Drug StudyCheezy BreadÎncă nu există evaluări
- Vesicovaginal Fistula: Urology DepartmentDocument24 paginiVesicovaginal Fistula: Urology DepartmentHardiTariqHamma100% (1)
- CBT Midwifery Full Mock Test 3 Questions Answers Numerical OrderDocument31 paginiCBT Midwifery Full Mock Test 3 Questions Answers Numerical OrderMimi BoamahÎncă nu există evaluări
- On LeukemiaDocument28 paginiOn LeukemiaMeena Koushal100% (1)
- Hypnoparenting Effects Towards Fatigue As An Impact of Chemotherapy Among Pediatric Patients With Acute Lymphoblastic LeukemiaDocument7 paginiHypnoparenting Effects Towards Fatigue As An Impact of Chemotherapy Among Pediatric Patients With Acute Lymphoblastic LeukemiaMuhammad HaezarÎncă nu există evaluări
- Fall From Heights Emergency Procedure - ACE CivilDocument1 paginăFall From Heights Emergency Procedure - ACE CivilNicole AnthonyÎncă nu există evaluări
- Williams Exercises Vs Mckenzie ExercisesDocument3 paginiWilliams Exercises Vs Mckenzie ExercisesMasi KhanÎncă nu există evaluări
- NFL Sideline Concussion Assessment TestDocument2 paginiNFL Sideline Concussion Assessment TestRobert LeeÎncă nu există evaluări
- NCM 112 Lec 1 Sir Arnel Respiratory System: Basic Gas-Exchange Unit of The RespiratoryDocument5 paginiNCM 112 Lec 1 Sir Arnel Respiratory System: Basic Gas-Exchange Unit of The RespiratoryJane BautistaÎncă nu există evaluări
- Ncp. Oral MucosaDocument1 paginăNcp. Oral MucosaZmiaÎncă nu există evaluări
- SCAT6 ToolDocument9 paginiSCAT6 ToolRobinÎncă nu există evaluări
- Relapsing Polychondritis - A 2016 Update On Clinical Features, Diagnostic Tools, Treatment and Biological Drug UseDocument18 paginiRelapsing Polychondritis - A 2016 Update On Clinical Features, Diagnostic Tools, Treatment and Biological Drug UseAldiÎncă nu există evaluări
- Biofeedback Therapy in Pune - Dr. Rupali Bandgar-JankarDocument3 paginiBiofeedback Therapy in Pune - Dr. Rupali Bandgar-JankardrrupalibandgarÎncă nu există evaluări
- Medical SpecialistsDocument2 paginiMedical SpecialistsArvin Dela CrÜzÎncă nu există evaluări
- Amnesic SyndromeDocument12 paginiAmnesic SyndromeMUHAMMAD BILALÎncă nu există evaluări
- Casts N TractionDocument3 paginiCasts N Tractionkatmarie14344100% (1)
- COVID 19 Quarantine Vs IsolationDocument1 paginăCOVID 19 Quarantine Vs IsolationBláck GhøstÎncă nu există evaluări
- Diabetes PathophysiologyDocument2 paginiDiabetes PathophysiologyRyan MulanoÎncă nu există evaluări
- Empiric Antibiotic ListDocument2 paginiEmpiric Antibiotic ListpasswordÎncă nu există evaluări
- Dr. Faiza Hashim SoomroDocument25 paginiDr. Faiza Hashim SoomroFaiza Hashim SoomroÎncă nu există evaluări
- PBL - Day 1 MSKDocument4 paginiPBL - Day 1 MSKAAGKhatriÎncă nu există evaluări
- Treatment of Colonic Diverticular Disease: Role of Surgery: Controversies in GastroenterologyDocument5 paginiTreatment of Colonic Diverticular Disease: Role of Surgery: Controversies in GastroenterologyGianfranco MuntoniÎncă nu există evaluări
- Acs OsceDocument4 paginiAcs OsceYohanes ArviÎncă nu există evaluări
- Leukemia CaseDocument28 paginiLeukemia CasehilalÎncă nu există evaluări
- Protocol TPEDocument19 paginiProtocol TPEPatricia TamasÎncă nu există evaluări
- What Are The Biological Agents That Can Be Utilized For Bioterrorism?Document30 paginiWhat Are The Biological Agents That Can Be Utilized For Bioterrorism?anukriti shrivastavaÎncă nu există evaluări