S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Question and Answers For MFD OSCE ExaminationDocument15 paginiQuestion and Answers For MFD OSCE ExaminationAmeer Fadel100% (1)
- Manual Terapia DigitalDocument38 paginiManual Terapia DigitalPaolaQuitian0% (1)
- TPNDocument69 paginiTPNMylz MendozaÎncă nu există evaluări
- Session 4-Tomato, SPepper, Brinjal PDFDocument71 paginiSession 4-Tomato, SPepper, Brinjal PDFHemanth Chowdary Alla0% (1)
- Nursing Care For BipolarDocument3 paginiNursing Care For BipolarAnthonyChapotin100% (2)
- Fractional RF Machine: Use InstructionDocument21 paginiFractional RF Machine: Use Instructionjuras500Încă nu există evaluări
- FinalDocument3 paginiFinalAnupam Saraf IIÎncă nu există evaluări
- Toriumi 2016Document7 paginiToriumi 2016Diego CuadrosÎncă nu există evaluări
- Case Study - 3 - Mumwa Crafts Association - Community Development Through Craft ProductionDocument29 paginiCase Study - 3 - Mumwa Crafts Association - Community Development Through Craft ProductionRifat HasanÎncă nu există evaluări
- 常用詞彙表Document10 pagini常用詞彙表GXÎncă nu există evaluări
- 1116005I Rev. 02Document2 pagini1116005I Rev. 02kirubel demelashÎncă nu există evaluări
- Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19) A ReviewDocument13 paginiPathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19) A ReviewBryan Diaz LopezÎncă nu există evaluări
- Annual Drug Data Report Vol-1 1971Document228 paginiAnnual Drug Data Report Vol-1 1971lasicablava50% (2)
- WBC CountingDocument4 paginiWBC CountingMarx AsuncionÎncă nu există evaluări
- Syrgery Mock 10Document8 paginiSyrgery Mock 10Sergiu CiobanuÎncă nu există evaluări
- Inggris 201Document5 paginiInggris 201hakimzainulÎncă nu există evaluări
- Urticaria and Angioedema: Bettina WediDocument26 paginiUrticaria and Angioedema: Bettina WediMerlin MuktialiÎncă nu există evaluări
- Chordoma Current Concepts Management and Future DirectionsDocument8 paginiChordoma Current Concepts Management and Future DirectionsChristian AdeÎncă nu există evaluări
- Reflection Paper Methodological Issues Associated Pharmacogenomic Biomarkers Relation Clinical - enDocument21 paginiReflection Paper Methodological Issues Associated Pharmacogenomic Biomarkers Relation Clinical - enmartin.dubuc-extÎncă nu există evaluări
- Gynae-L - MukundaDocument50 paginiGynae-L - MukundadocivirusÎncă nu există evaluări
- Peds 2015-3501 Full PDFDocument19 paginiPeds 2015-3501 Full PDFJehan VahlepyÎncă nu există evaluări
- Tracheal Intubation: Airway AssessmentDocument7 paginiTracheal Intubation: Airway AssessmentElle ReyesÎncă nu există evaluări
- b1 ChecklistDocument2 paginib1 ChecklistRoryÎncă nu există evaluări
- Test Planner-2022-2023 (CF+OYM) Phase-02 - FT, & TE Version 1.0-1Document4 paginiTest Planner-2022-2023 (CF+OYM) Phase-02 - FT, & TE Version 1.0-1Dev SoniÎncă nu există evaluări
- Tear and Pterygium A Clinicopathological Study of Conjunctiva For Tear Film Anomaly in PterygiumDocument7 paginiTear and Pterygium A Clinicopathological Study of Conjunctiva For Tear Film Anomaly in PterygiumShofi Dhia AiniÎncă nu există evaluări
- List COVID Facilities State OdishaDocument3 paginiList COVID Facilities State OdishadrjyotivetÎncă nu există evaluări
- Human Behavior & Crisis ManagementDocument74 paginiHuman Behavior & Crisis ManagementJvnRodz P GmlmÎncă nu există evaluări
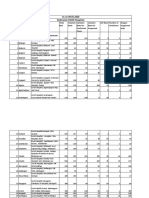
- Nairobi Morbidity 1st Qrt-2010-11Document49 paginiNairobi Morbidity 1st Qrt-2010-11Dominic KikuyuÎncă nu există evaluări
- Extensive Reading - AVK44CDocument42 paginiExtensive Reading - AVK44CNinh Nhat Thao Vy K189Încă nu există evaluări
- Summary Notes - Topic 14 Coordination and Response - CAIE Biology IGCSEDocument8 paginiSummary Notes - Topic 14 Coordination and Response - CAIE Biology IGCSEAmnaÎncă nu există evaluări