S-ar putea să vă placă și
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Absorbable Suture IndicationDocument57 paginiAbsorbable Suture IndicationSariSyamerÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Analysis of The Importance of The NHS Within Our Society ESSAYDocument16 paginiAnalysis of The Importance of The NHS Within Our Society ESSAYsophieloo_xÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
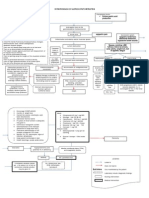
- Pathophysiology of GooDocument2 paginiPathophysiology of GooTania Noviza100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Air Liquide 2012en4275308938748421437Document63 paginiAir Liquide 2012en4275308938748421437Pushpa BaruaÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Tissue PerfusionDocument2 paginiTissue Perfusionnursezey100% (3)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- MMTDocument5 paginiMMTSharmin Chishty SusiwalaÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- PBLDocument2 paginiPBLarn0ld21Încă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Ms. Ann Female 48 Years Old Diabetes Mellitus Foot/diabetes Mellitus Joseph MDocument10 paginiMs. Ann Female 48 Years Old Diabetes Mellitus Foot/diabetes Mellitus Joseph MFielMendozaÎncă nu există evaluări
- Guías Infecciones Asociadas A Cateter IDSA 2009Document45 paginiGuías Infecciones Asociadas A Cateter IDSA 2009pablocaballiniÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Seminar Hippii Surabaya Peran Infection Prevention Control Nurse, Dalam MenghadapiDocument25 paginiSeminar Hippii Surabaya Peran Infection Prevention Control Nurse, Dalam MenghadapiHery SetiawanÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Clinical Trial Protocol TemplateDocument33 paginiClinical Trial Protocol TemplateNasilÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Burkitt LymphomaDocument13 paginiBurkitt LymphomaGalih Yogo0% (1)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Acumed ClavicleDocument6 paginiAcumed Claviclesiddig7Încă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- ResumeDocument2 paginiResumeapi-464603836Încă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Drug Study - ClonazepamDocument3 paginiDrug Study - ClonazepamJasmin Jacob80% (5)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Broken Arm DocumentDocument4 paginiBroken Arm DocumentJismy FregyÎncă nu există evaluări
- Perio Orto KokishDocument10 paginiPerio Orto KokishKARLA IBARRAÎncă nu există evaluări
- Angiographic ProjectionsDocument16 paginiAngiographic ProjectionsKarren_M888Încă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- NP 5Document12 paginiNP 5June DumdumayaÎncă nu există evaluări
- Scar Pocket RX PadDocument2 paginiScar Pocket RX Paderfaiz2Încă nu există evaluări
- Martin Lobatos Grand Jury IndictmentDocument14 paginiMartin Lobatos Grand Jury IndictmentNickÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Kavo1 1058 Primus MaintenanceDocument30 paginiKavo1 1058 Primus MaintenanceVoulgaris KostasÎncă nu există evaluări
- Referat Koass Interna Yarsi 11 SEPTEMBER 2017 - 9 NOVEMBER 2017Document2 paginiReferat Koass Interna Yarsi 11 SEPTEMBER 2017 - 9 NOVEMBER 2017Abiyya Farah Putri, MDÎncă nu există evaluări
- REG 195, Application For Disabled Person Placard or PlatesDocument3 paginiREG 195, Application For Disabled Person Placard or Platestech20000Încă nu există evaluări
- Standards For Digital Photography in Cranio-Maxillo-Facial Surgery - Part IIDocument12 paginiStandards For Digital Photography in Cranio-Maxillo-Facial Surgery - Part IIYeny BelÎncă nu există evaluări
- My Genes Made Me Do ItDocument19 paginiMy Genes Made Me Do ItMcshe Psych ClassÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- gl0087 PDFDocument58 paginigl0087 PDFNurul HikmahÎncă nu există evaluări
- Sample Supervision AgreementDocument1 paginăSample Supervision AgreementJohn GavazziÎncă nu există evaluări
- American Bar AssociationDocument6 paginiAmerican Bar AssociationMarkWarner100% (1)
- Nursing Manegmen of EQUIPMENTS in NICUDocument16 paginiNursing Manegmen of EQUIPMENTS in NICUPriyaÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)