S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Apoptotic Effects of CKD-602 and Cisplatin On OralDocument5 paginiApoptotic Effects of CKD-602 and Cisplatin On Oralpilyoungg1994Încă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Cyclin ADocument1 paginăCyclin Apilyoungg1994Încă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Prospective Study of Oral Cancer Provides Insight into Incidence, Risk Factors and Survival RatesDocument36 paginiProspective Study of Oral Cancer Provides Insight into Incidence, Risk Factors and Survival Ratespilyoungg1994Încă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- Dermabrasion Chemabrasion Laser ResurfacingDocument76 paginiDermabrasion Chemabrasion Laser Resurfacingpilyoungg1994100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- 필영 의국세 (02 2) (슬라이드)Document76 pagini필영 의국세 (02 2) (슬라이드)pilyoungg1994Încă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Lateral Thigh FlapDocument57 paginiLateral Thigh Flappilyoungg1994Încă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- 필영 외측대퇴 (구연)Document5 pagini필영 외측대퇴 (구연)pilyoungg1994Încă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
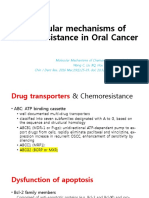
- Molecular Mechanisms of Chemoresistance in Oral CancerDocument8 paginiMolecular Mechanisms of Chemoresistance in Oral Cancerpilyoungg1994Încă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Effects of inflamed synovial fluid on iNOS and COX-2 in chondrocytesDocument18 paginiEffects of inflamed synovial fluid on iNOS and COX-2 in chondrocytespilyoungg1994Încă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- Ijms 22 08167 v3Document10 paginiIjms 22 08167 v3pilyoungg1994Încă nu există evaluări
- 상철-Neurophysiological Mechanisms of TMD (의국세) (01-1)Document48 pagini상철-Neurophysiological Mechanisms of TMD (의국세) (01-1)pilyoungg1994Încă nu există evaluări
- Tissue EngineeringDocument61 paginiTissue Engineeringpilyoungg1994Încă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- FaceliftDocument30 paginiFaceliftpilyoungg1994100% (1)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- RhinoDocument38 paginiRhinopilyoungg1994Încă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Local FlapDocument44 paginiLocal Flappilyoungg1994Încă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Indication and Perioperative Care of Surgical ExtractionDocument18 paginiIndication and Perioperative Care of Surgical Extractionpilyoungg1994Încă nu există evaluări
- Hair TransplantationDocument33 paginiHair Transplantationpilyoungg1994Încă nu există evaluări
- 이가편한세미나Document77 pagini이가편한세미나pilyoungg1994Încă nu există evaluări
- An Overview of the Prevention of Oral Cancer-석1신영민Document18 paginiAn Overview of the Prevention of Oral Cancer-석1신영민pilyoungg1994Încă nu există evaluări
- Bony Box Surgery For OSASDocument4 paginiBony Box Surgery For OSASpilyoungg1994Încă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Lateral Thigh FlapDocument57 paginiLateral Thigh Flappilyoungg1994Încă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- Comparison of Arthrocentesis and ArthroDocument38 paginiComparison of Arthrocentesis and Arthropilyoungg1994Încă nu există evaluări
- Capalbo A Et Al 2023 On The Reproductive Capabilities of Aneuploid Human Preimplantation EmbryosDocument10 paginiCapalbo A Et Al 2023 On The Reproductive Capabilities of Aneuploid Human Preimplantation EmbryosJorge Alberto Salazar CartinÎncă nu există evaluări
- Fungal Keratitis in FarmerDocument4 paginiFungal Keratitis in FarmerChikita Rizqi HanifatiÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Nephrotic/Nephritic Syndrome: AK. Soyibo Department of Medicine Review ClassDocument143 paginiNephrotic/Nephritic Syndrome: AK. Soyibo Department of Medicine Review ClassKay BristolÎncă nu există evaluări
- Management of The Urologic Sepsis SyndromeDocument10 paginiManagement of The Urologic Sepsis SyndromeNur Syamsiah MÎncă nu există evaluări
- Hip FractureDocument1 paginăHip FractureHAILIE23100% (3)
- Clsi 2012Document50 paginiClsi 2012niluh suwasanti100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Endovenous Microwave Ablation of Great Saphenous VeinDocument3 paginiEndovenous Microwave Ablation of Great Saphenous VeinMalekseuofi مالك السيوفيÎncă nu există evaluări
- Referral for dietitian assessment of swallowing riskDocument72 paginiReferral for dietitian assessment of swallowing riskjykaÎncă nu există evaluări
- Appendicitis and Crohn's Disease GuideDocument11 paginiAppendicitis and Crohn's Disease GuideJa DimasÎncă nu există evaluări
- Embryology MCQDocument10 paginiEmbryology MCQTofik MohammedÎncă nu există evaluări
- Clinical Practice Guideline for Pharmacologic Treatment of Chronic InsomniaDocument43 paginiClinical Practice Guideline for Pharmacologic Treatment of Chronic InsomniaAna Cristina BrazÎncă nu există evaluări
- Consent Form Nephrology BHUDocument6 paginiConsent Form Nephrology BHURajeshKumarJainÎncă nu există evaluări
- 2018 01 Early Pregnancy Loss LightDocument41 pagini2018 01 Early Pregnancy Loss LightMishal FatimaÎncă nu există evaluări
- Aconitum NapellusDocument12 paginiAconitum NapellusMuhammad Mustafa IjazÎncă nu există evaluări
- Classifications of Pharmaceutical Drugs1Document24 paginiClassifications of Pharmaceutical Drugs1RPh Krishna Chandra JagritÎncă nu există evaluări
- Njala University: Bo Campus-Kowama LocationDocument32 paginiNjala University: Bo Campus-Kowama LocationALLIEU FB SACCOHÎncă nu există evaluări
- Pre-Surgical Hand WashDocument2 paginiPre-Surgical Hand WashRatna LamaÎncă nu există evaluări
- Heat Illness Types, Causes, Symptoms and TreatmentsDocument46 paginiHeat Illness Types, Causes, Symptoms and TreatmentsDewi Pertiwi Pertiwi0% (1)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Organ Systems ComparisonDocument12 paginiOrgan Systems ComparisonJeffrey YumangÎncă nu există evaluări
- Peds Shelf NotesDocument88 paginiPeds Shelf Notesskeebs23100% (8)
- Managing Benign Breast ConditionsDocument20 paginiManaging Benign Breast Conditionschristel chadidÎncă nu există evaluări
- A5 Pig Management GuidlinesDocument4 paginiA5 Pig Management GuidlinesAnna NdunaÎncă nu există evaluări
- (Lecture) Approach To AscitesDocument48 pagini(Lecture) Approach To AscitesJirayu Puthhai100% (1)
- ACE2 Expression in Kidney and Testis May Cause Kidney and Testis Damage After 2019-nCoV InfectionDocument16 paginiACE2 Expression in Kidney and Testis May Cause Kidney and Testis Damage After 2019-nCoV InfectionSY LodhiÎncă nu există evaluări
- Talk WslidesDocument43 paginiTalk WslidesraydonalÎncă nu există evaluări
- HPNDocument4 paginiHPNFlorianne AdlawanÎncă nu există evaluări
- Combination of Lisinopril and Nifedipine GITS.10Document7 paginiCombination of Lisinopril and Nifedipine GITS.10Andi PermanaÎncă nu există evaluări
- Nutrients: Anemia of Chronic Diseases: Wider Diagnostics-Better Treatment?Document17 paginiNutrients: Anemia of Chronic Diseases: Wider Diagnostics-Better Treatment?Gufront MustofaÎncă nu există evaluări
- Notice To Employer (Final 5.2.24)Document12 paginiNotice To Employer (Final 5.2.24)Khasyafsufi AdminÎncă nu există evaluări
- New Microsoft Office Word DocumentDocument2 paginiNew Microsoft Office Word DocumentAnam BukhariÎncă nu există evaluări