S-ar putea să vă placă și
- Endodontic RadiologyDe la EverandEndodontic RadiologyBettina BasraniÎncă nu există evaluări
- Management of Deep Carious LesionDocument52 paginiManagement of Deep Carious LesionLaiba Asif RajputÎncă nu există evaluări
- Fundamentals of Oral and Maxillofacial RadiologyDe la EverandFundamentals of Oral and Maxillofacial RadiologyEvaluare: 4 din 5 stele4/5 (1)
- Lec5#Management of Deep Carious LesionsDocument46 paginiLec5#Management of Deep Carious LesionsMarwa TemirekÎncă nu există evaluări
- Smear LayerDocument13 paginiSmear LayerDental Spa100% (2)
- Smear LayerDocument36 paginiSmear LayerNaomi SinghÎncă nu există evaluări
- Cention N: Journal Club 3Document45 paginiCention N: Journal Club 3VaishnaviÎncă nu există evaluări
- Management of Deep Carious LesionsDocument5 paginiManagement of Deep Carious LesionsEmeka V. ObiÎncă nu există evaluări
- Space MaintainersDocument53 paginiSpace MaintainersAarti RelwaniÎncă nu există evaluări
- Management of Deep Carious Lesions in ChildrenDocument46 paginiManagement of Deep Carious Lesions in ChildrenSahil Gagnani100% (1)
- Smear LayerDocument114 paginiSmear LayerAME DENTAL COLLEGE RAICHUR, KARNATAKAÎncă nu există evaluări
- Band and LoopDocument129 paginiBand and LoopVijit Vadhyar100% (1)
- Composites in Pediatric Dentistry: ROLL NO. - 21277010001 Dr. Lopamoodra Das Batch-2018-2021Document20 paginiComposites in Pediatric Dentistry: ROLL NO. - 21277010001 Dr. Lopamoodra Das Batch-2018-2021Khushboorana A Scientist100% (1)
- Management of Discoloured Teeth: Presented By: Amisha Jain M.D.S II YearDocument44 paginiManagement of Discoloured Teeth: Presented By: Amisha Jain M.D.S II YearANUBHAÎncă nu există evaluări
- Space ManagementDocument14 paginiSpace ManagementWisam Layal A-sÎncă nu există evaluări
- Operative DentistryDocument51 paginiOperative Dentistryqra_beliebersÎncă nu există evaluări
- Tooth Coloured Restorative Materials FinalDocument166 paginiTooth Coloured Restorative Materials FinalAbhishek M AÎncă nu există evaluări
- New Microsoft PowerPoint PresentationDocument158 paginiNew Microsoft PowerPoint PresentationSutapa Roy100% (1)
- Dentin Bonding Agents - An OverviewDocument4 paginiDentin Bonding Agents - An OverviewIOSRjournalÎncă nu există evaluări
- 10-Apexogenesis & PulpectomyDocument5 pagini10-Apexogenesis & PulpectomyAhmed AbdÎncă nu există evaluări
- Diagnosis & Case Selection in EndodonticsDocument54 paginiDiagnosis & Case Selection in EndodonticsRawzh Salih MuhammadÎncă nu există evaluări
- Dentin Bonding AgentsDocument35 paginiDentin Bonding AgentsSatya Asatya0% (1)
- Irrigation of Root Canal: Assembled by Dr. Osama Asadi, B.D.SDocument35 paginiIrrigation of Root Canal: Assembled by Dr. Osama Asadi, B.D.SVizi AdrianÎncă nu există evaluări
- Abrasive Agents in DentistryDocument38 paginiAbrasive Agents in Dentistryjohn mwambu100% (1)
- Pulp CappingDocument59 paginiPulp CappingrisjunÎncă nu există evaluări
- Recent Advances in Endodontic Instruments / Orthodontic Courses by Indian Dental AcademyDocument20 paginiRecent Advances in Endodontic Instruments / Orthodontic Courses by Indian Dental Academyindian dental academy100% (2)
- Falp DesignDocument23 paginiFalp DesignAbdur RehmanÎncă nu există evaluări
- Investments of Dental MaterialsDocument30 paginiInvestments of Dental MaterialsAnnaAffandie100% (1)
- Endo EmergenciesDocument95 paginiEndo EmergenciesVincent SerÎncă nu există evaluări
- Dentinal HypersensitivityDocument75 paginiDentinal HypersensitivityMica BernardoÎncă nu există evaluări
- PulpDocument54 paginiPulpAnsh DuttaÎncă nu există evaluări
- Indirect and Direct Pulp Capping: Reactionary vs. Reparative DentinsDocument6 paginiIndirect and Direct Pulp Capping: Reactionary vs. Reparative Dentinshafizhuddin muhammadÎncă nu există evaluări
- Impression Techniques of FPDDocument20 paginiImpression Techniques of FPDBhavan Chand YemineniÎncă nu există evaluări
- Microbiology of Dental CariesDocument80 paginiMicrobiology of Dental Cariesdisha 146jandialÎncă nu există evaluări
- Dentinal Hypersensitivity: Dr. Nitin MaitinDocument133 paginiDentinal Hypersensitivity: Dr. Nitin MaitinShipra MaitinÎncă nu există evaluări
- Root Canal Sealers - SeminarDocument49 paginiRoot Canal Sealers - Seminarkowmudimaddineni100% (2)
- 1-2-3 Steps in Endodontic Irrigation PDFDocument4 pagini1-2-3 Steps in Endodontic Irrigation PDFAnn M.Încă nu există evaluări
- Restorative ResinsDocument23 paginiRestorative ResinsNaveen Kumar0% (1)
- Diseases of Periradicular TissuesDocument62 paginiDiseases of Periradicular Tissuesanubhutigupta1404Încă nu există evaluări
- Post Insertion InstructionsDocument23 paginiPost Insertion InstructionsAnkita Reddy VallapÎncă nu există evaluări
- Emergency Treatment in Endodontics: By: Mai Hamdy Ass. Prof. of Endodontics, Faculty of Dentistry, Suez Canal UniversityDocument70 paginiEmergency Treatment in Endodontics: By: Mai Hamdy Ass. Prof. of Endodontics, Faculty of Dentistry, Suez Canal Universitymahmoud100% (1)
- Non-Restorative Cavity TreatmentDocument8 paginiNon-Restorative Cavity TreatmentQurrat-ul-AinÎncă nu există evaluări
- Supportive Periodontal TherapyDocument53 paginiSupportive Periodontal TherapymenaxieÎncă nu există evaluări
- Regenerative Endodontics Part 2Document118 paginiRegenerative Endodontics Part 2rasagna reddyÎncă nu există evaluări
- Forces Acting On Restorations LD / Orthodontic Courses by Indian Dental AcademyDocument95 paginiForces Acting On Restorations LD / Orthodontic Courses by Indian Dental Academyindian dental academyÎncă nu există evaluări
- Tissue Conditioners and Soft LinersDocument71 paginiTissue Conditioners and Soft LinersSugandhi Pidaparthi100% (1)
- Impression Materials and Techniques in Fixed ProsthesisDocument116 paginiImpression Materials and Techniques in Fixed ProsthesisSharvaree100% (1)
- ApicoectomyDocument70 paginiApicoectomyCarlos Maglutac100% (2)
- Department of Conservative Dentistry: Presented By: Nikita GoyalDocument27 paginiDepartment of Conservative Dentistry: Presented By: Nikita GoyalAnkita GoyalÎncă nu există evaluări
- Biomechanics of Edentulous StateDocument30 paginiBiomechanics of Edentulous StateManash Jyoti DekaÎncă nu există evaluări
- Endodontic ErrorsDocument50 paginiEndodontic Errorsasop06Încă nu există evaluări
- Laminates and VennersDocument42 paginiLaminates and VennersJASPREETKAUR0410Încă nu există evaluări
- Cleaning & ShapingDocument47 paginiCleaning & ShapingdrmahmoudbadrÎncă nu există evaluări
- Cleaning and Shaping of Root Canal SystemDocument81 paginiCleaning and Shaping of Root Canal SystemToni MaddoxÎncă nu există evaluări
- Pit & Fissure SealantDocument49 paginiPit & Fissure SealantJessica AlexanderÎncă nu există evaluări
- Concepts of Enamel and Dentin AdhesionDocument12 paginiConcepts of Enamel and Dentin Adhesionizeldien5870Încă nu există evaluări
- Direct Indirect RetentionDocument11 paginiDirect Indirect RetentionMaha LakshmiÎncă nu există evaluări
- Full Coverage Restoration For Primary TeethDocument24 paginiFull Coverage Restoration For Primary TeethMohamed ElkafrawyÎncă nu există evaluări
- Amalgam BondingDocument21 paginiAmalgam BondingSaad Tanvir ShaikhÎncă nu există evaluări
- Pedo Long AnswerDocument116 paginiPedo Long AnswersamikshaÎncă nu există evaluări
- Reference Only: I Pus Pond StreetDocument132 paginiReference Only: I Pus Pond StreetJagdish ShindeÎncă nu există evaluări
- Pe Fir Handbook 1 2Document237 paginiPe Fir Handbook 1 2Salman JoÎncă nu există evaluări
- Cytech Products Data SheetsDocument71 paginiCytech Products Data Sheetslinga2014Încă nu există evaluări
- 410 Stainless Steel: Form of SupplyDocument3 pagini410 Stainless Steel: Form of SupplyDeepak SinghÎncă nu există evaluări
- Deepwater DrillingDocument54 paginiDeepwater DrillingQuag MireÎncă nu există evaluări
- Bioprocess Engineering 2Document1 paginăBioprocess Engineering 2asg rostÎncă nu există evaluări
- Effect of Flake Ice On Concrete CoolingDocument1 paginăEffect of Flake Ice On Concrete CoolingGianni TogniÎncă nu există evaluări
- GROUP 3 - LABORATORY REPORT 4 - Compounds With Hydroxyl GroupDocument18 paginiGROUP 3 - LABORATORY REPORT 4 - Compounds With Hydroxyl GroupJESSIE FREDRICK DALANIELÎncă nu există evaluări
- MMU 0102, MMA 0204, MMB 0207 - Professional: Vishay BeyschlagDocument13 paginiMMU 0102, MMA 0204, MMB 0207 - Professional: Vishay BeyschlagJan KowalskiÎncă nu există evaluări
- Isensee Robert W1943Document17 paginiIsensee Robert W1943DŨNG VŨ NGUYỄN TUẤNÎncă nu există evaluări
- Solutios, Solutions of Non Electrolyte - 2019-2020 v2Document80 paginiSolutios, Solutions of Non Electrolyte - 2019-2020 v2hazo hazÎncă nu există evaluări
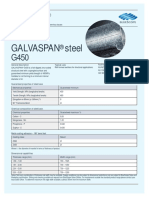
- Galvaspan G450Document2 paginiGalvaspan G450khurshedlakhoÎncă nu există evaluări
- TDS OF H-408 Silicone Adjuvant For AgricultureDocument2 paginiTDS OF H-408 Silicone Adjuvant For AgricultureAda FuÎncă nu există evaluări
- Introduction of Organic Chemistry by Eyes of Ajnish Kumar Gupta (AKG)Document24 paginiIntroduction of Organic Chemistry by Eyes of Ajnish Kumar Gupta (AKG)ajju_208180% (5)
- Potato Battery ExperimentDocument4 paginiPotato Battery Experimentvincent cuaÎncă nu există evaluări
- Solid-State Kinetic ModelsDocument14 paginiSolid-State Kinetic Modelsleizar_death64Încă nu există evaluări
- Light ExperimentsDocument12 paginiLight ExperimentsmamosÎncă nu există evaluări
- Product Information: Synpower™ Motor Oil Sae 5W-40Document2 paginiProduct Information: Synpower™ Motor Oil Sae 5W-40Iulia DanaÎncă nu există evaluări
- AMINE UNIT EVALUATION FORM Metric UnitDocument4 paginiAMINE UNIT EVALUATION FORM Metric Unitandrey.glinskyÎncă nu există evaluări
- Lesson Plan in Advanced Chemistry AlcohoDocument17 paginiLesson Plan in Advanced Chemistry AlcohoGlaiza Mapute CaringalÎncă nu există evaluări
- Welding Technology NotesDocument89 paginiWelding Technology NotesSanjay JangraÎncă nu există evaluări
- A Review On Natural Coagulants in Wastewater TreatmentDocument13 paginiA Review On Natural Coagulants in Wastewater Treatmentahsanur shuvoÎncă nu există evaluări
- PerforatingDocument65 paginiPerforatingdriller22100% (1)
- Hot-Dip Galvanization - WikipediaDocument4 paginiHot-Dip Galvanization - WikipediaaravindÎncă nu există evaluări
- Medidor Caudal Kobold Flotador UrkDocument4 paginiMedidor Caudal Kobold Flotador UrkBase SistemasÎncă nu există evaluări
- College of Nursing: Cebu Normal UniversityDocument5 paginiCollege of Nursing: Cebu Normal UniversityChelsea WuÎncă nu există evaluări
- To Achieve 100% 3D Printing Reliability: Our Easy Cheat SheetDocument7 paginiTo Achieve 100% 3D Printing Reliability: Our Easy Cheat Sheetfeere feeer0% (1)
- Component in Making Fiber Board As Substitute For HardiflexDocument9 paginiComponent in Making Fiber Board As Substitute For Hardiflexxiniac_1Încă nu există evaluări
- Factors Affecting Drug Absorption PDFDocument2 paginiFactors Affecting Drug Absorption PDFRobÎncă nu există evaluări
- Stoichiometry: Calculations With Chemical Formulas and EquationsDocument47 paginiStoichiometry: Calculations With Chemical Formulas and EquationsAngelo Miguel GarciaÎncă nu există evaluări