S-ar putea să vă placă și
- Pediatric OptometryDocument34 paginiPediatric OptometryUduma Kalu0% (1)
- Current Management of Diabetes MellitusDocument7 paginiCurrent Management of Diabetes MellitusVijayaletchumy ChandrashekaranÎncă nu există evaluări
- Preparat LabDocument1 paginăPreparat LabVijayaletchumy ChandrashekaranÎncă nu există evaluări
- K12 - Cell Injury (New)Document66 paginiK12 - Cell Injury (New)Vijayaletchumy ChandrashekaranÎncă nu există evaluări
- K7 - Diphtheria KBKDocument37 paginiK7 - Diphtheria KBKVijayaletchumy ChandrashekaranÎncă nu există evaluări
- Blok Oncology: Biochemistry Department Medical Faculty USUDocument40 paginiBlok Oncology: Biochemistry Department Medical Faculty USUJoelyn Fatima BurnardÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Temporomandibular Joint DisorderDocument9 paginiTemporomandibular Joint DisorderTannels100% (1)
- Malaria Control ProgramDocument17 paginiMalaria Control ProgramCaliso RichmondÎncă nu există evaluări
- Betamethasone (Drug Study)Document4 paginiBetamethasone (Drug Study)Franz.thenurse6888100% (1)
- 14 Proven Health Benefits of Guanabana (Soursop) Apart From Healing CancerDocument14 pagini14 Proven Health Benefits of Guanabana (Soursop) Apart From Healing CancerTerlumun JosephÎncă nu există evaluări
- Duke University Nurse Anesthesia Program (Acct #7042) Montgomery, Kelly Barton (Semester 7) Is Logged inDocument3 paginiDuke University Nurse Anesthesia Program (Acct #7042) Montgomery, Kelly Barton (Semester 7) Is Logged inkellyb11Încă nu există evaluări
- Practical Radiotherapy Planning, Fourth EditionDocument477 paginiPractical Radiotherapy Planning, Fourth EditionMehtap Coskun100% (12)
- Pneumatocele: BackgroundDocument8 paginiPneumatocele: BackgroundSilmi Noor RachniÎncă nu există evaluări
- Jurnal r5Document8 paginiJurnal r5Rezkina Azizah PutriÎncă nu există evaluări
- ConcorDocument40 paginiConcorviczÎncă nu există evaluări
- Zirconia ImplantsDocument15 paginiZirconia ImplantsmusatiiÎncă nu există evaluări
- Abnormal-Uterine-Bleeding Case StudyDocument57 paginiAbnormal-Uterine-Bleeding Case StudyOneForAll :100% (1)
- 16.MDR-XDR TBDocument18 pagini16.MDR-XDR TBLinna SriwaningsiÎncă nu există evaluări
- Drug Interactions in Psychiatry, 3rdDocument454 paginiDrug Interactions in Psychiatry, 3rdKhaled AbdelNaserÎncă nu există evaluări
- J Jacc 2023 04 019dDocument12 paginiJ Jacc 2023 04 019dCristi AlexandruÎncă nu există evaluări
- PT of The Shoulder PDFDocument573 paginiPT of The Shoulder PDFMuhammad Salman AzimÎncă nu există evaluări
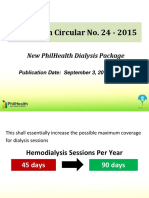
- 09 Dialysis DataDocument11 pagini09 Dialysis DataThinkingPinoyÎncă nu există evaluări
- Marketing Research MethodologyDocument3 paginiMarketing Research MethodologyAniket SinghÎncă nu există evaluări
- Funcional Properties of Bioctive Peptides Derived From MeatDocument22 paginiFuncional Properties of Bioctive Peptides Derived From MeatJohanna RomeroÎncă nu există evaluări
- DSM OcdDocument2 paginiDSM Ocdnmyza89Încă nu există evaluări
- En Do Tracheal SuctioningDocument30 paginiEn Do Tracheal Suctioningbalsam17Încă nu există evaluări
- Emergency Psychiatry Other Than Suicide: Dr. Pooja Singh, MD Assistant ProfessorDocument45 paginiEmergency Psychiatry Other Than Suicide: Dr. Pooja Singh, MD Assistant Professorpooja singhÎncă nu există evaluări
- BC DENTISTS-Abbreviated Fee GuideDocument2 paginiBC DENTISTS-Abbreviated Fee Guidewilliam_V_LeeÎncă nu există evaluări
- Jurnal AnemiaDocument4 paginiJurnal AnemiaAchmad Aidil TazakkaÎncă nu există evaluări
- CP - Hemophilia 2Document40 paginiCP - Hemophilia 2Reezka PutraÎncă nu există evaluări
- The Benefits of ExerciseDocument3 paginiThe Benefits of ExerciseAtet KurniadiÎncă nu există evaluări
- Nursing History Part 1. Demographic InformationDocument6 paginiNursing History Part 1. Demographic InformationAngelica VillalonÎncă nu există evaluări
- !!!-MBS Skin Item Numbers Nov 2016Document3 pagini!!!-MBS Skin Item Numbers Nov 2016abu ubaidahÎncă nu există evaluări
- Shigella: The Organism/ToxinDocument3 paginiShigella: The Organism/ToxinEduardo Ramirez LasoÎncă nu există evaluări
- Anxiety DisorderDocument9 paginiAnxiety DisorderSatish KujurÎncă nu există evaluări
- Intro CBTDocument12 paginiIntro CBTAria LevinsÎncă nu există evaluări