S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Safety Data Sheet: Chevron (Malaysia) Unleaded GasolineDocument12 paginiSafety Data Sheet: Chevron (Malaysia) Unleaded GasolineaminÎncă nu există evaluări
- Somatoform Disorders FinalDocument28 paginiSomatoform Disorders Finalapi-281484882Încă nu există evaluări
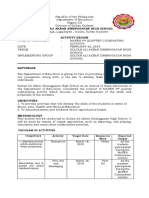
- Sultan Ali Akbar Sinenggayan High School: Program of Activities Activity Target Date Resources Need Expected OutputDocument5 paginiSultan Ali Akbar Sinenggayan High School: Program of Activities Activity Target Date Resources Need Expected OutputRAHIB SAMAYATINÎncă nu există evaluări
- q2 Grade 7 Health DLL Week 1Document8 paginiq2 Grade 7 Health DLL Week 1johann reyes0% (1)
- Drug Suffixes Cheat Sheet Sorted by Drug TypeDocument3 paginiDrug Suffixes Cheat Sheet Sorted by Drug TypeJennaÎncă nu există evaluări
- Meperidine Hydro ChlorideDocument4 paginiMeperidine Hydro Chlorideapi-3797941Încă nu există evaluări
- Valproate SodiumDocument2 paginiValproate SodiumKhairul KhairulÎncă nu există evaluări
- Physical Restraint Reduction For Older AdultsDocument11 paginiPhysical Restraint Reduction For Older Adultsantariksa tedyÎncă nu există evaluări
- Dwarfism: Navigation Search Dwarf (Germanic Mythology) DwarfDocument15 paginiDwarfism: Navigation Search Dwarf (Germanic Mythology) DwarfManzano JenecaÎncă nu există evaluări
- Recommendations For Cardiovascular Prevention DuringDocument5 paginiRecommendations For Cardiovascular Prevention DuringRaiyanÎncă nu există evaluări
- Carmen Best Background InformationDocument15 paginiCarmen Best Background InformationKING 5 NewsÎncă nu există evaluări
- Briearra Kennedy: University of Cincinnati, Cincinnati, OHDocument1 paginăBriearra Kennedy: University of Cincinnati, Cincinnati, OHapi-664515503Încă nu există evaluări
- Multigrade Lesson Plan in English3Document13 paginiMultigrade Lesson Plan in English3Nick Bantolo100% (11)
- IMPaCCT EU - Standards For Paediatric Palliative Care in EuropeDocument8 paginiIMPaCCT EU - Standards For Paediatric Palliative Care in EuropeSaraÎncă nu există evaluări
- Deped Naga City - Schools Division: Learning Activity Sheet No. 1 Quarter 1, HEALTH 8Document4 paginiDeped Naga City - Schools Division: Learning Activity Sheet No. 1 Quarter 1, HEALTH 8Jo DVera Gonzales IIÎncă nu există evaluări
- Myocardial Infarction: Disscused With Head Supervisor: DR - Yassmeen Ahmed of Pathology Department:prof - Dr.Manal El-NemrDocument23 paginiMyocardial Infarction: Disscused With Head Supervisor: DR - Yassmeen Ahmed of Pathology Department:prof - Dr.Manal El-NemrOmar ShazlyÎncă nu există evaluări
- Reviewer Micp Midterms 1Document29 paginiReviewer Micp Midterms 1Shiro KagomeÎncă nu există evaluări
- Benign Paroxysmal Positional VertigoDocument8 paginiBenign Paroxysmal Positional VertigoSubynk RidwanÎncă nu există evaluări
- Nursing Care Plan: Assessment Analysis Planning Implementation EvaluationDocument3 paginiNursing Care Plan: Assessment Analysis Planning Implementation EvaluationJeffrey LumacangÎncă nu există evaluări
- National Geographic March 2016Document148 paginiNational Geographic March 2016Anonymous Azxx3Kp9Încă nu există evaluări
- HYVC TTC Prospectus 2022 2023Document16 paginiHYVC TTC Prospectus 2022 2023Sreyashi BasuÎncă nu există evaluări
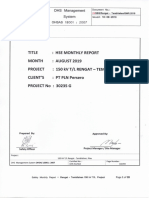
- SMR August 19 (Rengat - Tembilahan, Sect 2) PDFDocument28 paginiSMR August 19 (Rengat - Tembilahan, Sect 2) PDFDoo PLTGUÎncă nu există evaluări
- Borrescio-Higa Valenzuela - Gender Inequality and Mental Health.Document9 paginiBorrescio-Higa Valenzuela - Gender Inequality and Mental Health.Firdaus Silabi Al-AttarÎncă nu există evaluări
- Test Bank Health Assessment in Nursing 6th Edition Weber KelleyDocument9 paginiTest Bank Health Assessment in Nursing 6th Edition Weber KelleyPhyllis Vandenberge100% (25)
- Public Health in Community Settings: An IntroductionDocument22 paginiPublic Health in Community Settings: An IntroductionRusevÎncă nu există evaluări
- Clinical and Social Factors Associated With Violent Behavior in Persons With Schizophrenia Spectrum DisordersDocument6 paginiClinical and Social Factors Associated With Violent Behavior in Persons With Schizophrenia Spectrum DisordersIJAR JOURNALÎncă nu există evaluări
- A 6 Phlebitis and Infiltration ScalesDocument1 paginăA 6 Phlebitis and Infiltration ScalesSorin Alexandru LucaÎncă nu există evaluări
- Sexually Transmitted Diseases in MalesDocument15 paginiSexually Transmitted Diseases in MalesSam Raven AndresÎncă nu există evaluări
- RRL ExhalyzerDocument5 paginiRRL ExhalyzerKimberleigh MetrioÎncă nu există evaluări
- Laboratory Diagnosis of Bacterial Gastroenteritis: Romney M. Humphries, Andrea J. LinscottDocument29 paginiLaboratory Diagnosis of Bacterial Gastroenteritis: Romney M. Humphries, Andrea J. LinscottFatah Jati PÎncă nu există evaluări