S-ar putea să vă placă și
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesDe la EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesÎncă nu există evaluări
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Ed-Child Febrile FitDocument2 paginiEd-Child Febrile Fitmanish708345Încă nu există evaluări
- Paediatrics - Febrile Convulsions Assessment, Treatment and Education PDFDocument12 paginiPaediatrics - Febrile Convulsions Assessment, Treatment and Education PDFPalash NagdeoteÎncă nu există evaluări
- Therapeutic PlayDocument9 paginiTherapeutic PlayVivek PrabhakarÎncă nu există evaluări
- Minor Ailments of Newborn NewDocument47 paginiMinor Ailments of Newborn NewPOORNIMA B SÎncă nu există evaluări
- High Risk New BornDocument12 paginiHigh Risk New BornM. jehovah Nissie YeshalomeÎncă nu există evaluări
- Neonatal SeizuresDocument22 paginiNeonatal SeizuresKatrin Marcelina SihombingÎncă nu există evaluări
- Febrile Convulsions in ChildrenDocument2 paginiFebrile Convulsions in ChildrenMagdalena Dwiyani HutajuluÎncă nu există evaluări
- Iv TherapyDocument3 paginiIv TherapylovlyÎncă nu există evaluări
- Educational Competencies For Registered Nurses (MCIs)Document15 paginiEducational Competencies For Registered Nurses (MCIs)jasnate84100% (1)
- Acute Renal FailureDocument30 paginiAcute Renal FailureJerinÎncă nu există evaluări
- Promoting Nutritional Health During Pregnancy 19-20Document25 paginiPromoting Nutritional Health During Pregnancy 19-20Tony KhattarÎncă nu există evaluări
- Balance Diet Health Talk FinalDocument9 paginiBalance Diet Health Talk FinalRushikesh DigheÎncă nu există evaluări
- Spina Bifida ModuleDocument5 paginiSpina Bifida ModuleJulliza Joy PandiÎncă nu există evaluări
- Pregnancy Discomforts and InterventionsDocument37 paginiPregnancy Discomforts and Interventionspppamm100% (3)
- PnemoniaDocument38 paginiPnemoniaArjumand AliÎncă nu există evaluări
- Pyloric StenosisDocument2 paginiPyloric Stenosisgeorgeloto12Încă nu există evaluări
- Congenital Malformations of The New BornDocument14 paginiCongenital Malformations of The New BornMartha LubasiÎncă nu există evaluări
- Diarrhea: ChildrenDocument16 paginiDiarrhea: ChildrenEmmi Valentina PardedeÎncă nu există evaluări
- APPENDIX A-Normal Values in HumansDocument22 paginiAPPENDIX A-Normal Values in HumansSultan AlexandruÎncă nu există evaluări
- Prenatal Care by Connie Sussan AustenDocument31 paginiPrenatal Care by Connie Sussan AustenNoraÎncă nu există evaluări
- Oxygen Therapy and Oxygen Delivery (Pediatric) - CEDocument8 paginiOxygen Therapy and Oxygen Delivery (Pediatric) - CEViviana AltamiranoÎncă nu există evaluări
- Spina BifidaDocument10 paginiSpina BifidaMike Faustino SolangonÎncă nu există evaluări
- Minor Disorders of Newborn and Its ManagementDocument2 paginiMinor Disorders of Newborn and Its Managementsteffy sojan100% (1)
- Newborn CareDocument49 paginiNewborn CareJohn Mark PocsidioÎncă nu există evaluări
- HypothermiaDocument23 paginiHypothermiaKahfi Rakhmadian KiraÎncă nu există evaluări
- Management of Fever in ChildrenDocument1 paginăManagement of Fever in ChildrensabirÎncă nu există evaluări
- Nursing Care of at Risk/ High Risk/ Sick ClientDocument256 paginiNursing Care of at Risk/ High Risk/ Sick ClientAaron ConstantinoÎncă nu există evaluări
- Minordisordersofbnewborn 161129154708Document33 paginiMinordisordersofbnewborn 161129154708Kevin Daniel GoveasÎncă nu există evaluări
- Essential Newborn CareDocument67 paginiEssential Newborn CareTadesse MuhammedÎncă nu există evaluări
- Contraceptive Options For Women and Couples With HIV: Intrauterine Device (Iud or Iucd)Document23 paginiContraceptive Options For Women and Couples With HIV: Intrauterine Device (Iud or Iucd)Claudio UdjajaÎncă nu există evaluări
- Bladder Extrophy: Medical ManagementDocument8 paginiBladder Extrophy: Medical ManagementChristian James CamaongayÎncă nu există evaluări
- Care of Child Having Bladder Exstrophy and EpispadiasDocument3 paginiCare of Child Having Bladder Exstrophy and EpispadiasGarima ChaudharyÎncă nu există evaluări
- Immunization in New BornDocument5 paginiImmunization in New BornRose Lyn Camarista VelascoÎncă nu există evaluări
- Oral Manifestations of Nutritional Deficiency in Children PedoDocument29 paginiOral Manifestations of Nutritional Deficiency in Children PedoFourthMolar.com100% (1)
- 6-Health Problems Common in PreschoolerDocument36 pagini6-Health Problems Common in PreschoolerPam Lala100% (2)
- Neonatal Seizures and Management: Dhaka Sishu Hospital BangladeshDocument19 paginiNeonatal Seizures and Management: Dhaka Sishu Hospital BangladeshGoha BashaÎncă nu există evaluări
- Anatomy of The Female Pelvis: by DR. Zeinab Abotalib, MRCOG Associate Prof. of Obs & Gyn - King Saud UniversityDocument24 paginiAnatomy of The Female Pelvis: by DR. Zeinab Abotalib, MRCOG Associate Prof. of Obs & Gyn - King Saud UniversityThrishia Jade IgotÎncă nu există evaluări
- Hypothermia: Vandana ThakurDocument29 paginiHypothermia: Vandana ThakurRaja100% (1)
- Modern Concept of ChildcareDocument19 paginiModern Concept of ChildcareKiran Khasa0% (1)
- Diphtheria: By: Aguilloso, Shella Cano, Charnelle Jayne GDocument19 paginiDiphtheria: By: Aguilloso, Shella Cano, Charnelle Jayne Gjudith_carlosÎncă nu există evaluări
- Stage of Expulsion (2 Stage)Document36 paginiStage of Expulsion (2 Stage)Anonymous iG0DCOfÎncă nu există evaluări
- WelcomeDocument103 paginiWelcomeLyka BernalÎncă nu există evaluări
- Hydrocephalus Lesson Plan NewDocument18 paginiHydrocephalus Lesson Plan NewPinkymekala HasanparthyÎncă nu există evaluări
- Pregnancy ChangesDocument20 paginiPregnancy ChangesMj BrionesÎncă nu există evaluări
- Management of Patients With Neurologic DysfunctionDocument24 paginiManagement of Patients With Neurologic DysfunctionYahya AL-HelihÎncă nu există evaluări
- CholeraDocument4 paginiCholeraBeth AvelinoÎncă nu există evaluări
- Postmature Infants 1Document13 paginiPostmature Infants 1LyssaMarieKathryneEge100% (1)
- Baby Bath ChecklistDocument2 paginiBaby Bath ChecklistMomshie Felaih Binasoy Dela CruzÎncă nu există evaluări
- Hypertrophic Pyloric StenosisDocument23 paginiHypertrophic Pyloric StenosisRahel Imelda PanggabeanÎncă nu există evaluări
- Neonatal ProceduresDocument74 paginiNeonatal ProceduresIbrahim Sabra100% (1)
- 03.chronic Supp Otitis MediaDocument33 pagini03.chronic Supp Otitis MediaJumanne JayÎncă nu există evaluări
- Suppositories: Presented byDocument21 paginiSuppositories: Presented byVanessa PatraoÎncă nu există evaluări
- Common Neonatal Problems - 085835Document39 paginiCommon Neonatal Problems - 085835Jack AdamÎncă nu există evaluări
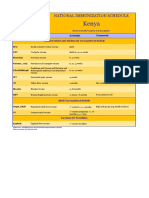
- Kenya Immunization ScheduleDocument1 paginăKenya Immunization ScheduleDani AnyikaÎncă nu există evaluări
- Protein Energy Malnutrition - 2Document32 paginiProtein Energy Malnutrition - 2J V SamuelÎncă nu există evaluări
- Hydrocephalus and Head Injury ......Document54 paginiHydrocephalus and Head Injury ......Rahul Dhaker100% (1)
- Postpartum Nursing PowerpointDocument3 paginiPostpartum Nursing PowerpointAntonella VitaleÎncă nu există evaluări
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Thrombocytopenia: What We Will Cover TodayDocument23 paginiThrombocytopenia: What We Will Cover TodayKimbek BuangkeÎncă nu există evaluări
- Perioperative Management OF Brain Trauma: Tatang Bisri Konsultan Neuroanestesi IDSAIDocument52 paginiPerioperative Management OF Brain Trauma: Tatang Bisri Konsultan Neuroanestesi IDSAIKimbek BuangkeÎncă nu există evaluări
- Neonatal SepsisDocument26 paginiNeonatal SepsisKimbek BuangkeÎncă nu există evaluări
- SY Crafts Christmas Hats&Cloth&Socks Price ListDocument16 paginiSY Crafts Christmas Hats&Cloth&Socks Price ListKimbek BuangkeÎncă nu există evaluări
- Diarrhoea in PediatricsDocument89 paginiDiarrhoea in PediatricsKimbek BuangkeÎncă nu există evaluări
- IkterusDocument14 paginiIkterusAji KristiantoÎncă nu există evaluări
- 5967 12818 1 SMDocument5 pagini5967 12818 1 SMKimbek BuangkeÎncă nu există evaluări
- Capacity (FVC) Pria Dewasa Denganoverweight: Pengaruh Latihan Aerobik Terhadap Forced VitalDocument6 paginiCapacity (FVC) Pria Dewasa Denganoverweight: Pengaruh Latihan Aerobik Terhadap Forced VitalKimbek BuangkeÎncă nu există evaluări
- RDA Chart RDA TableDocument4 paginiRDA Chart RDA TableVisshan SpirulinaÎncă nu există evaluări
- By Class - 11 (English) MM 60 TIME 2hr Mid-Term Examination SESSION - 202 Read The Following Passage Carefully: Fit To Fight (12m)Document3 paginiBy Class - 11 (English) MM 60 TIME 2hr Mid-Term Examination SESSION - 202 Read The Following Passage Carefully: Fit To Fight (12m)gunnÎncă nu există evaluări
- Thesis of Manjusha Sudha Devi (05.03.2021)Document180 paginiThesis of Manjusha Sudha Devi (05.03.2021)Chakrapani ChaturvediÎncă nu există evaluări
- 2MS File 3 Lesson PlansDocument17 pagini2MS File 3 Lesson PlansPearla WawaÎncă nu există evaluări
- Motto:Education Is The Best Legacy: Instructions: Choose A, B, C or D To Answer The Following Objective QuestionsDocument27 paginiMotto:Education Is The Best Legacy: Instructions: Choose A, B, C or D To Answer The Following Objective Questionsainomoh kayodeÎncă nu există evaluări
- Performance Task #1: A.Directions: Find Different Health Products You Use at Home, Write The Necessary Information AboutDocument4 paginiPerformance Task #1: A.Directions: Find Different Health Products You Use at Home, Write The Necessary Information AboutDYLAN ALESSANDRA FRANCISCOÎncă nu există evaluări
- Honoring God's Creation - Christianity and VegetarianismDocument16 paginiHonoring God's Creation - Christianity and VegetarianismVegan FutureÎncă nu există evaluări
- Natural Bioactive Compounds of Citrus Limon For Food and Health PDFDocument19 paginiNatural Bioactive Compounds of Citrus Limon For Food and Health PDFEsteban Davila100% (1)
- The Free McDougall ProgramDocument102 paginiThe Free McDougall ProgramLorrie100% (8)
- Nutrition Quiz Reviewer 1Document30 paginiNutrition Quiz Reviewer 1Prince Pascual Dela Cruz0% (1)
- Rations of The German Wehrmacht Change Update File 15oct10Document33 paginiRations of The German Wehrmacht Change Update File 15oct10Erwin Riefkogel100% (1)
- Nutritive Value of Fruits and VegetablesDocument25 paginiNutritive Value of Fruits and VegetablesSoumitra ParulekarÎncă nu există evaluări
- SPM Biology NotesDocument32 paginiSPM Biology NotesAin Fza0% (1)
- Imani-Lara Lansiquot Masterclass: Half Marathon Guide Shakes For DaysDocument70 paginiImani-Lara Lansiquot Masterclass: Half Marathon Guide Shakes For DaysArnav GautamÎncă nu există evaluări
- Wongs Essentials of Pediatric Nursing 10Th Edition Hockenberry Test Bank Full Chapter PDFDocument34 paginiWongs Essentials of Pediatric Nursing 10Th Edition Hockenberry Test Bank Full Chapter PDFdieulienheipgo100% (7)
- Importance of BiochemDocument19 paginiImportance of BiochemAmal100% (1)
- Ch-2 Components of Food Ppt-4Document14 paginiCh-2 Components of Food Ppt-4SUHANEERIYAÎncă nu există evaluări
- C10 - Food Technology. Challenge For HealthDocument9 paginiC10 - Food Technology. Challenge For HealthNguyễn Thị VươngÎncă nu există evaluări
- Fortimel Powder - Fact Sheet SA - FC PDFDocument2 paginiFortimel Powder - Fact Sheet SA - FC PDFUshal VeeriahÎncă nu există evaluări
- VitaminsDocument3 paginiVitaminsJayaprabhu PrabhuÎncă nu există evaluări
- CHAPTER 2 Literature ReviewDocument12 paginiCHAPTER 2 Literature ReviewAnas KamalÎncă nu există evaluări
- A2Z Chewable Product Information PageDocument3 paginiA2Z Chewable Product Information PageSamantha LopezÎncă nu există evaluări
- Ecce SampleDocument28 paginiEcce SampleSebastianÎncă nu există evaluări
- Journey of The First 1000 Days 25 - 04 - 2018 For Web (Low Res) PDFDocument177 paginiJourney of The First 1000 Days 25 - 04 - 2018 For Web (Low Res) PDFchandraprakash_shuklÎncă nu există evaluări
- HairFortin Reviews and Benefits - Health and MotivesDocument6 paginiHairFortin Reviews and Benefits - Health and MotivesHairFortin (2)Încă nu există evaluări
- Applied Nutrition Student Copy - Gr.12 - RajiDocument83 paginiApplied Nutrition Student Copy - Gr.12 - Rajinjood100% (1)
- Nutrition Concepts and Controversies 13Th Edition Sizer Test Bank Full Chapter PDFDocument33 paginiNutrition Concepts and Controversies 13Th Edition Sizer Test Bank Full Chapter PDFinlawbast.ileir100% (7)
- Plant Based Eating SPANDocument24 paginiPlant Based Eating SPANcamositaÎncă nu există evaluări
- Vitamin ADocument4 paginiVitamin AThunyapornÎncă nu există evaluări
- Chemistry 9 VitaminsDocument9 paginiChemistry 9 VitaminsKirstin LogronioÎncă nu există evaluări