S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Normal Spontaneous Vaginal DeliveryDocument41 paginiNormal Spontaneous Vaginal DeliveryDelphy Varghese100% (1)
- Treatment Plan TemplatesDocument2 paginiTreatment Plan TemplatesShalini Dass100% (3)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Geriatric Soap NoteDocument6 paginiGeriatric Soap Noteapi-282282363100% (6)
- Infectious QuestionDocument52 paginiInfectious Questionrayooona88Încă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Dear Reader, These Papers Were Meant To Be As An Extremely Quick Review and Ultra-Short Summary ofDocument9 paginiDear Reader, These Papers Were Meant To Be As An Extremely Quick Review and Ultra-Short Summary ofHazel D. Venus100% (2)
- Dear Reader, These Papers Were Meant To Be As An Extremely Quick Review and Ultra-Short Summary ofDocument9 paginiDear Reader, These Papers Were Meant To Be As An Extremely Quick Review and Ultra-Short Summary ofHazel D. Venus100% (2)
- DR Yayooo Novmber 2012 Expected Exam QuestionsDocument46 paginiDR Yayooo Novmber 2012 Expected Exam Questionsrayooona880% (1)
- April PrometricDocument26 paginiApril Prometricrayooona88100% (1)
- Dha & Scfhs ExamsDocument115 paginiDha & Scfhs Examsrayooona88100% (4)
- Tranexamic Acid Indications and ContraindicationsDocument27 paginiTranexamic Acid Indications and ContraindicationsMallikarjunÎncă nu există evaluări
- Tranexamic Acid Indications and ContraindicationsDocument27 paginiTranexamic Acid Indications and ContraindicationsMallikarjunÎncă nu există evaluări
- Dha Prometric Feb-3 ShabeerDocument2 paginiDha Prometric Feb-3 ShabeerDr-Usman KhanÎncă nu există evaluări
- Fluid and Electrolyte Nursing Care Management 112Document7 paginiFluid and Electrolyte Nursing Care Management 112anne marieÎncă nu există evaluări
- Rubrics For Preparing Blood TransfusionDocument4 paginiRubrics For Preparing Blood TransfusionMARK JOSHUA ALFAROÎncă nu există evaluări
- MSM Brochure PDFDocument14 paginiMSM Brochure PDFLinda Kayser100% (2)
- AntibioticsDocument10 paginiAntibioticsJulián David Ríos ZuluagaÎncă nu există evaluări
- AntidoteDocument1 paginăAntidoterayooona88Încă nu există evaluări
- Pharmaceutical Excipients - Where Do We Begin?Document3 paginiPharmaceutical Excipients - Where Do We Begin?rayooona88Încă nu există evaluări
- AB ClassesDocument4 paginiAB Classesrayooona88100% (2)
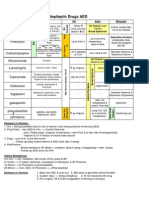
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocument1 paginăAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Încă nu există evaluări
- Formulas Related Question, PebcDocument1 paginăFormulas Related Question, PebcBhavesh NidhiÎncă nu există evaluări
- Study On Effect of Wet Cupping (Hijama) On Blood Lipid Profile in Human at Aldyssah-Alshati, LibyaDocument4 paginiStudy On Effect of Wet Cupping (Hijama) On Blood Lipid Profile in Human at Aldyssah-Alshati, LibyaMohammed Ramzy GhifariÎncă nu există evaluări
- Detrusor InstabilityDocument7 paginiDetrusor Instabilityapi-3705046Încă nu există evaluări
- Cells in The PBSDocument31 paginiCells in The PBSDelzell Dame CasaneÎncă nu există evaluări
- MCQ MedicineDocument4 paginiMCQ MedicineKasun PereraÎncă nu există evaluări
- Jurnal KurapDocument3 paginiJurnal Kurapbunga farnadaÎncă nu există evaluări
- PRIO Lemus Acute Pain and Risk For Def. Fluid VolumeDocument3 paginiPRIO Lemus Acute Pain and Risk For Def. Fluid VolumeChe ValenzuelaÎncă nu există evaluări
- Cheatsheet PDFDocument2 paginiCheatsheet PDFJudaeo SandovalÎncă nu există evaluări
- Non-ST Elevation Myocardial Infarction (NSTEMI) Case ReportDocument28 paginiNon-ST Elevation Myocardial Infarction (NSTEMI) Case ReportuculucullÎncă nu există evaluări
- Female Anatomy ExplainedDocument11 paginiFemale Anatomy ExplainedBARRIENTOS, RITCHELLE C.Încă nu există evaluări
- Number of Workers (Fill Total Number of Workers For Each Sub-Contractor at Work Daily) No - Sub-Contractor No. of Workers Suke Ca3Document8 paginiNumber of Workers (Fill Total Number of Workers For Each Sub-Contractor at Work Daily) No - Sub-Contractor No. of Workers Suke Ca3Nazulaila WitraÎncă nu există evaluări
- Defek Septum Atrium: PJB Asianotik Shunt Dari Atrium Kiri Ke KananDocument10 paginiDefek Septum Atrium: PJB Asianotik Shunt Dari Atrium Kiri Ke KananFrida Neila RahmatikaÎncă nu există evaluări
- EctopicDocument4 paginiEctopicAb Staholic BoiiÎncă nu există evaluări
- Preeclampsia and PregnancyDocument1 paginăPreeclampsia and PregnancyirmaÎncă nu există evaluări
- Marks-100: Model Exam: English & Personality Enhancement Program Duration - 3 HrsDocument6 paginiMarks-100: Model Exam: English & Personality Enhancement Program Duration - 3 HrsSunil MukundanÎncă nu există evaluări
- Skeletal TractionDocument11 paginiSkeletal Tractionpolarbear121212Încă nu există evaluări
- Impact of Self-Management Education on Diabetes PatientsDocument3 paginiImpact of Self-Management Education on Diabetes PatientsArief AndriyantoÎncă nu există evaluări
- Intro V2-2Document5 paginiIntro V2-2KKKÎncă nu există evaluări
- Kumpulan Refarat Co-Ass Radiologi FK UntarDocument15 paginiKumpulan Refarat Co-Ass Radiologi FK UntarErwin DiprajaÎncă nu există evaluări
- Recipe FormatDocument1 paginăRecipe FormatScribdTranslationsÎncă nu există evaluări
- Fundamentals of Rheumatoid Arthritis and Various Homoeopathic Trials in Patients of Rheumatoid Arthritis: An UpdateDocument6 paginiFundamentals of Rheumatoid Arthritis and Various Homoeopathic Trials in Patients of Rheumatoid Arthritis: An UpdateHomoeopathic PulseÎncă nu există evaluări
- 2023 - Registration FormDocument3 pagini2023 - Registration FormhusnanabiyyuÎncă nu există evaluări
- Central Singapore GP Clinic ListDocument236 paginiCentral Singapore GP Clinic Listnash hanaÎncă nu există evaluări
- Vit A DeficiencyDocument27 paginiVit A DeficiencyNatnaelÎncă nu există evaluări
- PDF PPT Drug AbuseDocument16 paginiPDF PPT Drug AbuseRandom personÎncă nu există evaluări