S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- 10 Anthony Varos PDFDocument134 pagini10 Anthony Varos PDFbadar_aqÎncă nu există evaluări
- Article7 13 4 PDFDocument6 paginiArticle7 13 4 PDFbadar_aqÎncă nu există evaluări
- Macro EconomicsDocument90 paginiMacro EconomicsshahidkakaÎncă nu există evaluări
- Article7 13 4 PDFDocument6 paginiArticle7 13 4 PDFbadar_aqÎncă nu există evaluări
- 10 Anthony Varos PDFDocument134 pagini10 Anthony Varos PDFbadar_aqÎncă nu există evaluări
- Clinical: New Dentures From Old: A Duplication Method Using "Appropriatech"Document5 paginiClinical: New Dentures From Old: A Duplication Method Using "Appropriatech"badar_aqÎncă nu există evaluări
- 10 Anthony Varos PDFDocument134 pagini10 Anthony Varos PDFbadar_aqÎncă nu există evaluări
- Head+and+neck Mcqs With AnswersDocument178 paginiHead+and+neck Mcqs With Answersbadar_aqÎncă nu există evaluări
- MDS Operative DentistryDocument4 paginiMDS Operative Dentistrybadar_aqÎncă nu există evaluări
- Module-1: General Introduction M1: General Introduction M1.1 Introduction of CompositesDocument35 paginiModule-1: General Introduction M1: General Introduction M1.1 Introduction of CompositesAÎncă nu există evaluări
- Brainstem DetailedDocument157 paginiBrainstem Detailedbadar_aqÎncă nu există evaluări
- Cortex and Limbic SystemDocument26 paginiCortex and Limbic Systembadar_aqÎncă nu există evaluări
- Clinical: New Dentures From Old: A Duplication Method Using "Appropriatech"Document5 paginiClinical: New Dentures From Old: A Duplication Method Using "Appropriatech"badar_aqÎncă nu există evaluări
- First Aid Anatomy Notes PDFDocument15 paginiFirst Aid Anatomy Notes PDFbadar_aqÎncă nu există evaluări
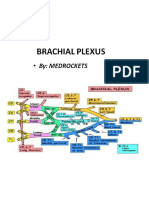
- Brachial PlexusDocument30 paginiBrachial Plexusbadar_aqÎncă nu există evaluări
- Nbde 1 Test 1Document45 paginiNbde 1 Test 1badar_aqÎncă nu există evaluări
- Nbde I 2010Document4 paginiNbde I 2010badar_aqÎncă nu există evaluări
- MDS Operative Dentistry PDFDocument4 paginiMDS Operative Dentistry PDFbadar_aqÎncă nu există evaluări
- Monday - Anatomy Tuesday - Biochemistry Wednesday - Physiology Thursday - Pathology Friday - Microbiology Saturday - Dental AnatomyDocument1 paginăMonday - Anatomy Tuesday - Biochemistry Wednesday - Physiology Thursday - Pathology Friday - Microbiology Saturday - Dental Anatomybadar_aqÎncă nu există evaluări
- Ore Reading ListDocument3 paginiOre Reading Listupul85Încă nu există evaluări
- Master's in Clinical Dentistry (MClinDent) EndodontologyDocument8 paginiMaster's in Clinical Dentistry (MClinDent) Endodontologybadar_aqÎncă nu există evaluări
- Application Checklist Fellowship in Dental Surgery Without ExaminationDocument1 paginăApplication Checklist Fellowship in Dental Surgery Without Examinationbadar_aqÎncă nu există evaluări
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- MJDF Revision Course Pt1 Flyer 150314Document1 paginăMJDF Revision Course Pt1 Flyer 150314badar_aqÎncă nu există evaluări
- Sample NOT FOR Reproduction: Impacted CaninesDocument2 paginiSample NOT FOR Reproduction: Impacted Caninesbadar_aqÎncă nu există evaluări
- BJOS v2 n4 141 143Document3 paginiBJOS v2 n4 141 143badar_aqÎncă nu există evaluări
- Unit Wise Lectures LDocument278 paginiUnit Wise Lectures Lbadar_aqÎncă nu există evaluări
- MJDF Revision Course Pt1 Flyer 150314Document1 paginăMJDF Revision Course Pt1 Flyer 150314badar_aqÎncă nu există evaluări
- MJDF OscesDocument37 paginiMJDF Oscesbadar_aqÎncă nu există evaluări
- ExodontiaDocument24 paginiExodontiabadar_aqÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Somera CaseDocument5 paginiSomera Caseoceaneagles06Încă nu există evaluări
- Tufts Pharmacology ReviewDocument46 paginiTufts Pharmacology Reviewtesh_sachdeva100% (3)
- Chapter 15 Local AnestheticsDocument27 paginiChapter 15 Local AnestheticskmcalleÎncă nu există evaluări
- Synthesis of Procaine PDFDocument3 paginiSynthesis of Procaine PDFLive FlightsÎncă nu există evaluări
- LocalanestheticsDocument51 paginiLocalanestheticskingkb4uÎncă nu există evaluări
- Local Anesthesia Drugs CDA 2006 MalamedDocument6 paginiLocal Anesthesia Drugs CDA 2006 MalamedSaj1985100% (2)
- Pharmacology of Local AnestheticsDocument25 paginiPharmacology of Local AnestheticsMonica RaafatÎncă nu există evaluări
- MCQ Pharmacology No CommentDocument137 paginiMCQ Pharmacology No CommentYego EdwinÎncă nu există evaluări
- Lecture05c. (Note ) Classification of Oral AnesthesiaDocument55 paginiLecture05c. (Note ) Classification of Oral AnesthesiaDrMohmed MostafaÎncă nu există evaluări
- Procaine VeterinaryDocument4 paginiProcaine VeterinaryadezepÎncă nu există evaluări
- Somera CaseDocument2 paginiSomera CaseLiezzel Jeanette GorospeÎncă nu există evaluări
- Drugstudy NorocaineDocument2 paginiDrugstudy NorocaineMsOrangeÎncă nu există evaluări
- Local Anesthesia For The Dental Hygienist - Ebook (PDFDrive)Document680 paginiLocal Anesthesia For The Dental Hygienist - Ebook (PDFDrive)Joyce Ebol100% (2)
- TUFTS PharmacologyDocument20 paginiTUFTS PharmacologyMr. FarrahÎncă nu există evaluări
- Topic 10 The Pharmarceutical Industries L1Document13 paginiTopic 10 The Pharmarceutical Industries L1Yong LiÎncă nu există evaluări
- Amines and AmidesDocument24 paginiAmines and AmidesAzura Aziz100% (1)
- The Medical Student S Anesthesia PocketbookDocument16 paginiThe Medical Student S Anesthesia Pocketbookmarianaalvim100% (1)
- MCQ PharmacologyDocument278 paginiMCQ PharmacologyNader Almaswary0% (1)
- Cardiovascular DrugsDocument4 paginiCardiovascular DrugsSanjay Shirodkar100% (1)
- Tufts PharmacologyDocument46 paginiTufts Pharmacologykalicoj100% (5)
- Classification of Local AnestheticsDocument50 paginiClassification of Local AnestheticsHelen Reyes HallareÎncă nu există evaluări
- MCQs LADocument29 paginiMCQs LAPadmavathi C100% (1)
- The Somera CaseDocument3 paginiThe Somera CaseJacob ReyesÎncă nu există evaluări
- NYSORA - The New York School of Regional Anesthesia - Spinal Anesthesia - ContinuedDocument16 paginiNYSORA - The New York School of Regional Anesthesia - Spinal Anesthesia - ContinuedPatrick RetengÎncă nu există evaluări
- Method of Vital Extirpation PDFDocument23 paginiMethod of Vital Extirpation PDFShany SchwarzwaldÎncă nu există evaluări
- Local AnestheticsDocument45 paginiLocal AnestheticsAubrey Monette Padilla-ItchonÎncă nu există evaluări
- Oral Surgery Board ReviewDocument26 paginiOral Surgery Board ReviewmirfanulhaqÎncă nu există evaluări
- Local Anesthesia - DR - Ibrahim - ShaikhDocument101 paginiLocal Anesthesia - DR - Ibrahim - ShaikhDrIbrahimShaikhÎncă nu există evaluări
- Local Anaesthesia in EndodonticsDocument76 paginiLocal Anaesthesia in Endodonticssaurav kumar duttaÎncă nu există evaluări
- Local AnesthesiaDocument55 paginiLocal AnesthesiaAhmed MagdyÎncă nu există evaluări