S-ar putea să vă placă și
- Diagnostics I - PulsesDocument15 paginiDiagnostics I - Pulsesg23164100% (1)
- Presenting: (Diclofenac Diethylamine B.P. 100 MG)Document2 paginiPresenting: (Diclofenac Diethylamine B.P. 100 MG)drprasantÎncă nu există evaluări
- Advised Rest and If Required Low Intensity Light Activities During The Period of T/T of 10-12 DaysDocument2 paginiAdvised Rest and If Required Low Intensity Light Activities During The Period of T/T of 10-12 Daysdrprasant100% (1)
- Presenting: (Ketoprofen I.P. 20 MG)Document2 paginiPresenting: (Ketoprofen I.P. 20 MG)drprasantÎncă nu există evaluări
- Clinic Theater 2 - Class 4Document2 paginiClinic Theater 2 - Class 4drprasantÎncă nu există evaluări
- Clinic Theater 2 - Class 5Document2 paginiClinic Theater 2 - Class 5drprasant100% (1)
- Disorders of LobesDocument55 paginiDisorders of LobesdrprasantÎncă nu există evaluări
- Given The Code in The Exhibit What Is The Result? A. B. C. D. Answer: B Explanation: ZDocument1 paginăGiven The Code in The Exhibit What Is The Result? A. B. C. D. Answer: B Explanation: ZdrprasantÎncă nu există evaluări
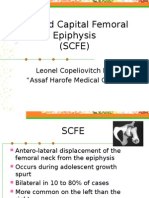
- Slipped Capital Femoral EpiphysisDocument12 paginiSlipped Capital Femoral EpiphysisdrprasantÎncă nu există evaluări
- PNF and Other TechniquesDocument8 paginiPNF and Other TechniquesdrprasantÎncă nu există evaluări
- Ebook NPTE TipsDocument11 paginiEbook NPTE Tipsdrprasant100% (1)
- Capri Institute of Manual Therapy: Address For Correspondence: - A-64, Hans Apartment, East Arjun Nagar, CBDDocument1 paginăCapri Institute of Manual Therapy: Address For Correspondence: - A-64, Hans Apartment, East Arjun Nagar, CBDdrprasantÎncă nu există evaluări
- Manipulation Therapy For Tennis Elbow:-: Prasant Gupta BPT Final YearDocument2 paginiManipulation Therapy For Tennis Elbow:-: Prasant Gupta BPT Final YeardrprasantÎncă nu există evaluări
- KiblerDocument10 paginiKiblerdrprasantÎncă nu există evaluări
- Neural Mobilizations (By David Butler) : How To Stretch A Nerve???Document1 paginăNeural Mobilizations (By David Butler) : How To Stretch A Nerve???drprasantÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Jaa 178927 Approaches To The Assessment of Severe Asthma Barriers and PDFDocument17 paginiJaa 178927 Approaches To The Assessment of Severe Asthma Barriers and PDFNikki LangatoÎncă nu există evaluări
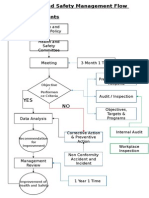
- Health and Safety FlowDocument6 paginiHealth and Safety Flowzaki0304Încă nu există evaluări
- Learning Plan Nursing PregradDocument3 paginiLearning Plan Nursing Pregradapi-25180064033% (3)
- KodefDocument45 paginiKodefWann FarhannaÎncă nu există evaluări
- Q& A DelegationDocument11 paginiQ& A DelegationFilipino Nurses CentralÎncă nu există evaluări
- Sequalae of Wearing Complete DenturesDocument34 paginiSequalae of Wearing Complete DenturesAyeshaAslamÎncă nu există evaluări
- Melanoma Skin Cancer Early Detection, Diagnosis, and StagingDocument21 paginiMelanoma Skin Cancer Early Detection, Diagnosis, and StagingKristine YoungÎncă nu există evaluări
- TFN ReviewerDocument18 paginiTFN Reviewerkiki park100% (1)
- CASP Case Control Study Checklist 2018 - Fillable - Form PDFDocument6 paginiCASP Case Control Study Checklist 2018 - Fillable - Form PDFEllieÎncă nu există evaluări
- The Newcastle Upon Tyne Hospitals NHS Foundation Trust Asepsis PolicyDocument10 paginiThe Newcastle Upon Tyne Hospitals NHS Foundation Trust Asepsis Policyyousrazeidan1979Încă nu există evaluări
- NCM109Document4 paginiNCM109Cherry Ann Cagayat MadrigalÎncă nu există evaluări
- SexDocument4 paginiSexQuotes&Anecdotes100% (1)
- Thesis About Quack DoctorsDocument22 paginiThesis About Quack DoctorsJervyn Guianan100% (3)
- InfluenzaDocument7 paginiInfluenzaGionne Carlo GomezÎncă nu există evaluări
- Communication Skills in MedicineDocument5 paginiCommunication Skills in MedicineSGD blima semlimanamÎncă nu există evaluări
- Cmca Activity 1 AliamenDocument5 paginiCmca Activity 1 AliamenJasmine AliamenÎncă nu există evaluări
- Free Online Courses WebsitesDocument27 paginiFree Online Courses Websitespervez4356Încă nu există evaluări
- Discharge SummaryDocument5 paginiDischarge SummaryNatarajan Palani88% (8)
- 5 Minute Anxiety Relief TechniquesDocument1 pagină5 Minute Anxiety Relief TechniquesBhettoh OrtizÎncă nu există evaluări
- NEBOSH IG1 Open Book Mock Examination For Sept. 2022Document5 paginiNEBOSH IG1 Open Book Mock Examination For Sept. 2022m.naÎncă nu există evaluări
- Infectious Diseases of The Female Genital TractDocument1.111 paginiInfectious Diseases of The Female Genital TractJohn Ntokos100% (2)
- Intradermal Delivery Vaccines Report 2009 SeptDocument94 paginiIntradermal Delivery Vaccines Report 2009 SeptSantoso CokroÎncă nu există evaluări
- Pathogen Reduction/Hazard Analysis Critical Control Point (HACCP) Systems Final Rule 9 CFR Part 417Document16 paginiPathogen Reduction/Hazard Analysis Critical Control Point (HACCP) Systems Final Rule 9 CFR Part 417Mili MartinezÎncă nu există evaluări
- Unit 01 OTHMDocument45 paginiUnit 01 OTHMsam100% (4)
- Community Health NursingDocument14 paginiCommunity Health Nursingyasira0% (1)
- Curahealth Hospitals Completes The Purchase of Specialty Hospital of JacksonvilleDocument2 paginiCurahealth Hospitals Completes The Purchase of Specialty Hospital of JacksonvillePR.comÎncă nu există evaluări
- Immunization HandbookDocument200 paginiImmunization Handbooktakumikuroda100% (1)
- Medical MarijuanaDocument4 paginiMedical MarijuanaDanielZepedaPereaÎncă nu există evaluări
- How Is The Effect of Health Services On Toddler Diarrhea?: Ecological Analysis in IndonesiaDocument11 paginiHow Is The Effect of Health Services On Toddler Diarrhea?: Ecological Analysis in IndonesiaomniyaÎncă nu există evaluări
- Pan India Network ListDocument230 paginiPan India Network ListParag RautÎncă nu există evaluări