S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- ManuscriptDocument14 paginiManuscriptAnonymous y6NmP9NHkYÎncă nu există evaluări
- ManuscriptDocument17 paginiManuscriptAnonymous y6NmP9NHkYÎncă nu există evaluări
- An Overview of Referral Patients With Severe Preeclampsia in Obstetric and Gynecology Department, Dr. Soetomo Hospital Surabaya in 2011 An OverviewDocument10 paginiAn Overview of Referral Patients With Severe Preeclampsia in Obstetric and Gynecology Department, Dr. Soetomo Hospital Surabaya in 2011 An OverviewAnonymous y6NmP9NHkYÎncă nu există evaluări
- Surat Kesediaan First Author Under Review Akhir November 2018Document6 paginiSurat Kesediaan First Author Under Review Akhir November 2018Anonymous y6NmP9NHkYÎncă nu există evaluări
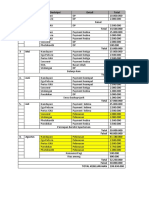
- Timeline RABDocument1 paginăTimeline RABAnonymous y6NmP9NHkYÎncă nu există evaluări
- Curriculum Vitae: Faisal Yusuf Ashari, MDDocument3 paginiCurriculum Vitae: Faisal Yusuf Ashari, MDAnonymous y6NmP9NHkYÎncă nu există evaluări
- Systemic Lupus Eritematus Kuliah KlerkDocument76 paginiSystemic Lupus Eritematus Kuliah KlerkAnonymous y6NmP9NHkYÎncă nu există evaluări
- High Tuberculosis Notification and Treatment Success Rates Through Community Participation in Central Sulawesi, Republic of IndonesiaDocument8 paginiHigh Tuberculosis Notification and Treatment Success Rates Through Community Participation in Central Sulawesi, Republic of IndonesiaAnonymous y6NmP9NHkYÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Chapter 6 Test Skeletal SystemDocument49 paginiChapter 6 Test Skeletal SystemAlexandra CampeanuÎncă nu există evaluări
- Chapter 14 SkeletonDocument6 paginiChapter 14 SkeletonJian Leong ThoÎncă nu există evaluări
- Transporte Óseo. Julio de PablosDocument48 paginiTransporte Óseo. Julio de PablosNuno Craveiro LopesÎncă nu există evaluări
- Baumgaertner. The Value of The Tip-Apex Distance PDFDocument8 paginiBaumgaertner. The Value of The Tip-Apex Distance PDFIcaruscignusÎncă nu există evaluări
- 02 The Nose and The Associated StructuresDocument72 pagini02 The Nose and The Associated Structuresmalaths757Încă nu există evaluări
- Congenital Talipes Equinovarus FinalDocument28 paginiCongenital Talipes Equinovarus FinalTibin Kavumkal ThomasÎncă nu există evaluări
- 2023 JOT Low Transcondylar Fractures of The Distal Humerus - A Multicenter Cohort StudyDocument6 pagini2023 JOT Low Transcondylar Fractures of The Distal Humerus - A Multicenter Cohort StudyjcmarecauxlÎncă nu există evaluări
- Morning Report: Pembimbing: Dr. Djunifer Hasudungan Sagala, Sp. OT (K) Dr. Andreas Wahyu W, Sp. OTDocument55 paginiMorning Report: Pembimbing: Dr. Djunifer Hasudungan Sagala, Sp. OT (K) Dr. Andreas Wahyu W, Sp. OTSinda AgathaÎncă nu există evaluări
- MilwaukeeDocument24 paginiMilwaukeeRiaz UddinÎncă nu există evaluări
- 2006 TMJ Hylander CorrectedDocument33 pagini2006 TMJ Hylander CorrectedKrupali JainÎncă nu există evaluări
- George MCQ 2010Document9 paginiGeorge MCQ 2010Mohamad RamadanÎncă nu există evaluări
- Arthur Macgregor, 1985, Bone Antler, İvory, HornDocument64 paginiArthur Macgregor, 1985, Bone Antler, İvory, Hornmustafa sarışahinÎncă nu există evaluări
- Chapter 6 Skeletal System OutlineDocument4 paginiChapter 6 Skeletal System OutlineIsabelle TanÎncă nu există evaluări
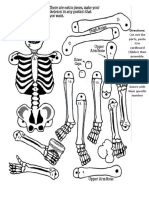
- Skeletal System ActivityDocument1 paginăSkeletal System ActivityChristopher UrbinoÎncă nu există evaluări
- MuscleDocument6 paginiMuscleMariel AbatayoÎncă nu există evaluări
- Bones of The Shoulder Are The HumerusDocument4 paginiBones of The Shoulder Are The HumerusHello RainbowÎncă nu există evaluări
- Corrected Ortho QsDocument48 paginiCorrected Ortho QsMuhamad Danial Kholili Al-JaloriÎncă nu există evaluări
- Neuraxial AnaesthesiaDocument12 paginiNeuraxial Anaesthesiakl;kzÎncă nu există evaluări
- Subaxial Cervical Spine Trauma: Evaluation and Surgical Decision-MakingDocument7 paginiSubaxial Cervical Spine Trauma: Evaluation and Surgical Decision-Makingvicky174Încă nu există evaluări
- Xii Neet Locomotion LDocument9 paginiXii Neet Locomotion LShagufta100% (1)
- Nomina AnatomicaDocument4 paginiNomina AnatomicaIoana Purice100% (1)
- Chapter 11 - Skeletal System Morphophys - 2020 - The Zebrafish in Biomedical ResDocument6 paginiChapter 11 - Skeletal System Morphophys - 2020 - The Zebrafish in Biomedical ResNicolas BaronÎncă nu există evaluări
- Test Bank For Anatomy Physiology An Integrative Approach 4th Edition Michael Mckinley Valerie Oloughlin Theresa BidleDocument110 paginiTest Bank For Anatomy Physiology An Integrative Approach 4th Edition Michael Mckinley Valerie Oloughlin Theresa Bidlejavierdoyleafkqexcgzj100% (31)
- The HandDocument4 paginiThe HandRoland Garcia Pelagio Jr.Încă nu există evaluări
- Pocket Atlas of Radiographic Anatomy 21-30Document10 paginiPocket Atlas of Radiographic Anatomy 21-30Ivan Alejandro Gonzalez DiazÎncă nu există evaluări
- Desarrollo de La Enf. Segmento ADYACENTE.2006: March 2014Document9 paginiDesarrollo de La Enf. Segmento ADYACENTE.2006: March 2014J Alan SantosÎncă nu există evaluări
- Perthes Disease: Mohamed Hamood MohamedDocument4 paginiPerthes Disease: Mohamed Hamood MohamedMohamed HamoodÎncă nu există evaluări
- MRI of The Whole BodyDocument276 paginiMRI of The Whole BodyfysmaÎncă nu există evaluări
- FocusOn WristArthritisDocument5 paginiFocusOn WristArthritisNicholas Raphael JohanÎncă nu există evaluări
- Bones - LabDocument24 paginiBones - LabJhom Andrei Apolinar100% (1)