S-ar putea să vă placă și
- Anatomy and Physiology of The Cardiovascular System Medical Surgical NursingDocument68 paginiAnatomy and Physiology of The Cardiovascular System Medical Surgical NursingFelix NjakeÎncă nu există evaluări
- Cardiac CycleDocument38 paginiCardiac CycleKok HoongÎncă nu există evaluări
- Pathology+101 Complete)Document147 paginiPathology+101 Complete)Goh Kah Yong100% (2)
- Cardiac Cycle by Bala GoyalDocument14 paginiCardiac Cycle by Bala Goyaltee su lingÎncă nu există evaluări
- Electrical Conduction in The HeartDocument35 paginiElectrical Conduction in The HeartNormasnizam Mohd NoorÎncă nu există evaluări
- Heart Anatomy: LocationDocument45 paginiHeart Anatomy: LocationZaira100% (1)
- Thyroid Disorder PDFDocument324 paginiThyroid Disorder PDFsuci w100% (2)
- Self-Administered EFT (Emotional Freedom Techniques) in Individuals With Fibromyalgia: A Randomized TrialDocument6 paginiSelf-Administered EFT (Emotional Freedom Techniques) in Individuals With Fibromyalgia: A Randomized TrialInnoVision Health Media100% (1)
- Cardiac Physiology PDFDocument17 paginiCardiac Physiology PDFAli Aborges Jr.Încă nu există evaluări
- Circulatory SystemDocument304 paginiCirculatory Systemyapyihao2100% (1)
- Cardiac CycleDocument30 paginiCardiac CycleCarrine Liew100% (2)
- Cardaic DrugsDocument57 paginiCardaic DrugsJyoti KathwalÎncă nu există evaluări
- Sensation and Perception HandoutsDocument3 paginiSensation and Perception HandoutsMariaMirandaJrÎncă nu există evaluări
- Cardiac CycleDocument31 paginiCardiac CycleAdwaitha KrÎncă nu există evaluări
- Cardio SlidesDocument309 paginiCardio SlidesGina VasquezÎncă nu există evaluări
- Total LaryngectomyDocument15 paginiTotal LaryngectomyKumaran Bagavathi RagavanÎncă nu există evaluări
- Lecture On Cardiac Cycle by DR RoomiDocument43 paginiLecture On Cardiac Cycle by DR RoomiMudassar Roomi100% (2)
- Cardiac Cycle FinalDocument37 paginiCardiac Cycle Finalindra_jeet2009Încă nu există evaluări
- Foundation of Nursing Practice Exam For Nursing Process Physical and Health Assessment and Routine ProceduresDocument24 paginiFoundation of Nursing Practice Exam For Nursing Process Physical and Health Assessment and Routine ProceduresAdrian Miguel100% (1)
- Basics of Cath LabDocument121 paginiBasics of Cath LabizalxrayÎncă nu există evaluări
- 2 Hemodynamic Theory On SICPDocument62 pagini2 Hemodynamic Theory On SICPantoni_gamundi3942Încă nu există evaluări
- Brief Readings SWEDENBORG's PSYCHOLOGY Howard Davis Spoerl Swedenborg Foundation 1937Document16 paginiBrief Readings SWEDENBORG's PSYCHOLOGY Howard Davis Spoerl Swedenborg Foundation 1937francis batt100% (1)
- Cancer PainDocument52 paginiCancer PainIndraYudhi100% (1)
- HypospadiaDocument45 paginiHypospadiaMartha P100% (1)
- HypospadiaDocument45 paginiHypospadiaMartha P100% (1)
- Adv Acu Tech 1 - The Second Metacarpal Bone TherapyDocument24 paginiAdv Acu Tech 1 - The Second Metacarpal Bone Therapysuperser123465100% (2)
- Transfer To Definitive Care EcaDocument40 paginiTransfer To Definitive Care EcaFahrurido Kusbari100% (1)
- Patent Ductus Arteriosus: by Dr. Hanan Zekri Khaled Lecturer of Pediatrics Pediatric CardiologyDocument36 paginiPatent Ductus Arteriosus: by Dr. Hanan Zekri Khaled Lecturer of Pediatrics Pediatric CardiologyEira RajkumarÎncă nu există evaluări
- Apley's System of Orthopaedics and Fractures 9th Edition PDFDocument993 paginiApley's System of Orthopaedics and Fractures 9th Edition PDFInggriht Senny Bondang96% (53)
- Heart As A Pump: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraDocument33 paginiHeart As A Pump: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraXeniel AlastairÎncă nu există evaluări
- K - 12 Heart As A Pump (Fisiologi)Document36 paginiK - 12 Heart As A Pump (Fisiologi)missirenaÎncă nu există evaluări
- Oral PathologyDocument23 paginiOral PathologyRuba AbbassÎncă nu există evaluări
- Cvs PPT 2) BpehssDocument35 paginiCvs PPT 2) BpehssAmbreen GhafoorÎncă nu există evaluări
- 3 Cardiology HemodynamicsDocument90 pagini3 Cardiology HemodynamicsPravallika ReddyÎncă nu există evaluări
- Cardiovascular Physiology: October 25, 2010Document51 paginiCardiovascular Physiology: October 25, 2010VinuPrakashJ.Încă nu există evaluări
- KP 1.3.2.1 Aktivitas Mekanik Jantung (2 Jam)Document68 paginiKP 1.3.2.1 Aktivitas Mekanik Jantung (2 Jam)Try MutiaraÎncă nu există evaluări
- PC Cardiac CycleDocument29 paginiPC Cardiac CycleSebontu HasenÎncă nu există evaluări
- The HeartDocument65 paginiThe HeartMichael SamaniegoÎncă nu există evaluări
- Lecture-5 Cardiac CycleDocument28 paginiLecture-5 Cardiac Cyclettalhalatif99Încă nu există evaluări
- The Cardiac Cycle: Dr. Abdalla Adam AbdallaDocument15 paginiThe Cardiac Cycle: Dr. Abdalla Adam AbdallaNimisha BalakrishnanÎncă nu există evaluări
- The Cardiac Cycle: Dr. Abdalla Adam AbdallaDocument15 paginiThe Cardiac Cycle: Dr. Abdalla Adam AbdallaNimisha BalakrishnanÎncă nu există evaluări
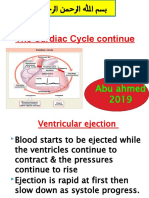
- The Cardiac Cycle Continue: Abu Ahmed 2019Document19 paginiThe Cardiac Cycle Continue: Abu Ahmed 2019Khalid AbdullahÎncă nu există evaluări
- The Cardiac Cycle Continue: Abu Ahmed 2019Document19 paginiThe Cardiac Cycle Continue: Abu Ahmed 2019Khalid AbdullahÎncă nu există evaluări
- Amboss - Cradiac CycleDocument18 paginiAmboss - Cradiac CycleAllysahÎncă nu există evaluări
- Cardiac Cycle CardiodynamicsDocument29 paginiCardiac Cycle Cardiodynamicseverforyou2023Încă nu există evaluări
- Cv-4 PHDocument28 paginiCv-4 PHaya najemÎncă nu există evaluări
- Cardiac Cycle: DR Rakesh JainDocument97 paginiCardiac Cycle: DR Rakesh JainKemoy FrancisÎncă nu există evaluări
- The Cardiac CycleDocument19 paginiThe Cardiac CycleRebi NesroÎncă nu există evaluări
- Review of HemodynanicsDocument17 paginiReview of HemodynanicsNoel V. ImmaculataÎncă nu există evaluări
- Cardiovascular PhysiologyDocument88 paginiCardiovascular Physiologykhorrami4Încă nu există evaluări
- Prof DR Najneen AkhterDocument62 paginiProf DR Najneen Akhterislamamirul0487Încă nu există evaluări
- Anatomy 10 - 01 - 18 PosteDocument19 paginiAnatomy 10 - 01 - 18 PosteOlga KucinskaÎncă nu există evaluări
- Cardiac SystemDocument5 paginiCardiac SystemTanya TuckerÎncă nu există evaluări
- 04-The Cardiac Cycle - Wigger's Diagram (J Swanevelder)Document6 pagini04-The Cardiac Cycle - Wigger's Diagram (J Swanevelder)Patrick WilliamsÎncă nu există evaluări
- The Cardiac Cycle 2Document7 paginiThe Cardiac Cycle 2Abigail ChristisnÎncă nu există evaluări
- Cardio Notes 1Document8 paginiCardio Notes 1Lindsay Grace MandarioÎncă nu există evaluări
- Cardiac CycleDocument4 paginiCardiac CycleDivya RanasariaÎncă nu există evaluări
- Cardiovascular SystemDocument6 paginiCardiovascular SystemJeminah Fae CalmaÎncă nu există evaluări
- Physiology of The HeartDocument38 paginiPhysiology of The HeartPanasheÎncă nu există evaluări
- CARDIAC CYCLE-laDocument12 paginiCARDIAC CYCLE-latehillahkabwe100Încă nu există evaluări
- Cardiac CycleDocument30 paginiCardiac CycleAdel100% (1)
- Cardiovascular Physiology: Lawrence A. Olatunji ReaderDocument46 paginiCardiovascular Physiology: Lawrence A. Olatunji ReaderMaryam Ogunade0% (1)
- CV Physio-IntroductionDocument33 paginiCV Physio-IntroductionHanaÎncă nu există evaluări
- Cardiac CycleDocument18 paginiCardiac CycleKundan GuptaÎncă nu există evaluări
- Study FastDocument49 paginiStudy FastmbbsporalekhaÎncă nu există evaluări
- Anatomy and Physiology of The Heart: Dr. N. PraveenDocument56 paginiAnatomy and Physiology of The Heart: Dr. N. Praveenamjad khan100% (1)
- Heart and CirculationDocument63 paginiHeart and CirculationNuraina SakinaÎncă nu există evaluări
- Cardiac Cycle: DR Rida Ajmal KhanDocument29 paginiCardiac Cycle: DR Rida Ajmal KhanMooma fatimaÎncă nu există evaluări
- Cardiac Cycle: Dr. Arun Goel Associate Professor Department of PhysiologyDocument27 paginiCardiac Cycle: Dr. Arun Goel Associate Professor Department of PhysiologyThird Year B PharmÎncă nu există evaluări
- 2014 Kuliah Fisiologi JantungDocument102 pagini2014 Kuliah Fisiologi JantungAlfia NadiraÎncă nu există evaluări
- Y2 Week 2 Aortic StenosisDocument4 paginiY2 Week 2 Aortic Stenosissurreal_blankÎncă nu există evaluări
- Transport in Humans 2 Heart and Cardiac CycleDocument74 paginiTransport in Humans 2 Heart and Cardiac Cycleloycoy008Încă nu există evaluări
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideDe la EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideÎncă nu există evaluări
- AppendicitisDocument10 paginiAppendicitisNaikko80Încă nu există evaluări
- 1 ManagementDocument5 pagini1 ManagementIndraYudhiÎncă nu există evaluări
- Tumor Ginjal + Lapkas PasienDocument3 paginiTumor Ginjal + Lapkas PasienIndraYudhiÎncă nu există evaluări
- Tumor Ginjal + Lapkas PasienDocument3 paginiTumor Ginjal + Lapkas PasienIndraYudhiÎncă nu există evaluări
- Tumor GinjalDocument5 paginiTumor GinjalIndraYudhiÎncă nu există evaluări
- Tumor Ginjal + Lapkas PasienDocument3 paginiTumor Ginjal + Lapkas PasienIndraYudhiÎncă nu există evaluări
- Change in The Concentration of Urolithiasis Markers Depending On The Degree of Activity of Stone Formation in Patients With Recurrent Stone DiseaseDocument4 paginiChange in The Concentration of Urolithiasis Markers Depending On The Degree of Activity of Stone Formation in Patients With Recurrent Stone DiseaseIndraYudhiÎncă nu există evaluări
- Atlas Akses VaskulerDocument77 paginiAtlas Akses VaskulerMuhammad Nor RifaniÎncă nu există evaluări
- Identi Fication of Synovial Fluid Biomarkers For Knee Osteoarthritis and Correlation With Radiographic AssessmentDocument6 paginiIdenti Fication of Synovial Fluid Biomarkers For Knee Osteoarthritis and Correlation With Radiographic AssessmentIndraYudhiÎncă nu există evaluări
- Change in The Concentration of Urolithiasis Markers Depending On The Degree of Activity of Stone Formation in Patients With Recurrent Stone DiseaseDocument4 paginiChange in The Concentration of Urolithiasis Markers Depending On The Degree of Activity of Stone Formation in Patients With Recurrent Stone DiseaseIndraYudhiÎncă nu există evaluări
- Dangerous Doctor in Pain ManagementDocument54 paginiDangerous Doctor in Pain ManagementIndraYudhiÎncă nu există evaluări
- Vertebral Fractures: Clinical PracticeDocument9 paginiVertebral Fractures: Clinical PracticeIndraYudhiÎncă nu există evaluări
- Change in The Concentration of Urolithiasis Markers Depending On The Degree of Activity of Stone Formation in Patients With Recurrent Stone DiseaseDocument4 paginiChange in The Concentration of Urolithiasis Markers Depending On The Degree of Activity of Stone Formation in Patients With Recurrent Stone DiseaseIndraYudhiÎncă nu există evaluări
- Single-Incision Thoracoscopic Surgery For PrimaryDocument4 paginiSingle-Incision Thoracoscopic Surgery For PrimaryIndraYudhiÎncă nu există evaluări
- Antiurolithiatic Activity of Daucus Carota: An in Vitro StudyDocument5 paginiAntiurolithiatic Activity of Daucus Carota: An in Vitro StudyIndraYudhiÎncă nu există evaluări
- Antiurolithiatic Activity of Daucus Carota: An in Vitro StudyDocument5 paginiAntiurolithiatic Activity of Daucus Carota: An in Vitro StudyIndraYudhiÎncă nu există evaluări
- Endourology and Stones Does Hypertension Impact 24-Hour Urine Parameters in Patients With Nephrolithiasis?Document5 paginiEndourology and Stones Does Hypertension Impact 24-Hour Urine Parameters in Patients With Nephrolithiasis?IndraYudhiÎncă nu există evaluări
- Vertebral Fractures: Clinical PracticeDocument9 paginiVertebral Fractures: Clinical PracticeIndraYudhiÎncă nu există evaluări
- Acute Cardiac CareDocument41 paginiAcute Cardiac CareIndraYudhiÎncă nu există evaluări
- The Influence of Oral Medication in Improving Physiccal Fitness and FlexibilityDocument40 paginiThe Influence of Oral Medication in Improving Physiccal Fitness and FlexibilityIndraYudhiÎncă nu există evaluări
- Ijms 16 11903Document63 paginiIjms 16 11903satyagraha84Încă nu există evaluări
- Amputatic InjuryDocument16 paginiAmputatic InjuryIndraYudhiÎncă nu există evaluări
- AINSDocument60 paginiAINSIndraYudhiÎncă nu există evaluări
- Susunan Peredaran Darah ManusiaDocument42 paginiSusunan Peredaran Darah ManusiaIndraYudhiÎncă nu există evaluări
- The Influence of Oral Medication in Improving Physiccal Fitness and FlexibilityDocument40 paginiThe Influence of Oral Medication in Improving Physiccal Fitness and FlexibilityIndraYudhiÎncă nu există evaluări
- The Rational Pain Treatment Risk of Un-Appropriate Pain TreatmentDocument37 paginiThe Rational Pain Treatment Risk of Un-Appropriate Pain TreatmentIndraYudhiÎncă nu există evaluări
- The Effect of Nacl 0.9% and Nacl 0.45% On Sodium, Chloride, and Acid - Base Balance in A Picu PopulationDocument7 paginiThe Effect of Nacl 0.9% and Nacl 0.45% On Sodium, Chloride, and Acid - Base Balance in A Picu Populationzack dahlanÎncă nu există evaluări
- Unit 5.: Facultad de Medicina Humana "Daniel Alcides Carrión Garcia"Document12 paginiUnit 5.: Facultad de Medicina Humana "Daniel Alcides Carrión Garcia"MARCOABADÎncă nu există evaluări
- Mitsunori M, Kagayaki K, Satoshi Y, Akihiro H, Naokazu H, Ken T, Hideki A, and Takatoshi SDocument14 paginiMitsunori M, Kagayaki K, Satoshi Y, Akihiro H, Naokazu H, Ken T, Hideki A, and Takatoshi SJasper CubiasÎncă nu există evaluări
- The Independence of Combinatory Semantic Processing: Evidence From Event-Related PotentialsDocument21 paginiThe Independence of Combinatory Semantic Processing: Evidence From Event-Related Potentialsdkm2030Încă nu există evaluări
- NCP 1Document1 paginăNCP 1hsiriaÎncă nu există evaluări
- The Effects of High-Velocity, Low-Amplitude Manipulation and Muscle Energy Technique On Suboccipital TendernessDocument8 paginiThe Effects of High-Velocity, Low-Amplitude Manipulation and Muscle Energy Technique On Suboccipital TendernessFlávio GuimarãesÎncă nu există evaluări
- Knight, Angela - The VampdomDocument8 paginiKnight, Angela - The VampdomLaviniaÎncă nu există evaluări
- تقرير ثرموداينمكDocument5 paginiتقرير ثرموداينمكاحمد كاظمÎncă nu există evaluări
- TIMI Score For NSTEMI, STEMI and Unstable AnginaDocument8 paginiTIMI Score For NSTEMI, STEMI and Unstable AnginaBenny TrisaktyariÎncă nu există evaluări
- Biological (Met)Document52 paginiBiological (Met)SirLhitz B. UmaliÎncă nu există evaluări
- 5CRMSDocument2 pagini5CRMSpandoraelitesÎncă nu există evaluări
- Ineffective Airway Clearance NCPDocument1 paginăIneffective Airway Clearance NCPBenz ParCoÎncă nu există evaluări
- Voice Disorder 2011 PDFDocument6 paginiVoice Disorder 2011 PDFfaidgustisyarifÎncă nu există evaluări
- Acute Effects of Tissue Flossing On Ankle Range of Motion and Tensiomyography Parameter - Matjaz Vogrin 2021Document8 paginiAcute Effects of Tissue Flossing On Ankle Range of Motion and Tensiomyography Parameter - Matjaz Vogrin 2021YngaMarquezJairÎncă nu există evaluări
- Manage Chest TubesDocument75 paginiManage Chest TubesWillington CuaresmaÎncă nu există evaluări
- 1987 Liophis - Green Species of South America - Dixon PDFDocument20 pagini1987 Liophis - Green Species of South America - Dixon PDFLuis VillegasÎncă nu există evaluări
- Chloride & Protein in CSF: Biochemistry Lab - 3 StageDocument19 paginiChloride & Protein in CSF: Biochemistry Lab - 3 Stagebknmy2nx9qÎncă nu există evaluări
- Bio Quiz BeeDocument2 paginiBio Quiz BeeRuchi Briam James LagitnayÎncă nu există evaluări