S-ar putea să vă placă și
- Urinary Tract Infection in Children - Classification, Diagnosis and TreatmentDe la EverandUrinary Tract Infection in Children - Classification, Diagnosis and TreatmentÎncă nu există evaluări
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Pancytopenia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandPancytopenia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Problem-based Approach to Gastroenterology and HepatologyDe la EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisÎncă nu există evaluări
- Anaemia in Pregnancy: By-Dr. Soumya.p (2nd Yr PG) Mod - Dr. Rita. D (Professor and Hod)Document98 paginiAnaemia in Pregnancy: By-Dr. Soumya.p (2nd Yr PG) Mod - Dr. Rita. D (Professor and Hod)SoumyaÎncă nu există evaluări
- RicketsDocument3 paginiRicketsLoverMind CabaronÎncă nu există evaluări
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsDe la EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsÎncă nu există evaluări
- Masalah Gastrointestinal KolestasisDocument21 paginiMasalah Gastrointestinal KolestasisMuthi'ah Ramadhani AgusÎncă nu există evaluări
- Infant Jaundice, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandInfant Jaundice, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsEvaluare: 5 din 5 stele5/5 (1)
- Anemia in ChildrenDocument9 paginiAnemia in ChildrenVillegas Sepúlveda AbrahamÎncă nu există evaluări
- Hemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUDocument27 paginiHemorrhagic Conditions in Neonates: DR Hodan Ahmed, Department of Pediatrics and Child Health, Amoud Medical School, AUAbdisalan hassanÎncă nu există evaluări
- WHO Manual - The Treatment of DiarrhoeaDocument47 paginiWHO Manual - The Treatment of DiarrhoeaRamona BunescuÎncă nu există evaluări
- Abdominal Mass Differential PresentationDocument42 paginiAbdominal Mass Differential Presentationdeb haartÎncă nu există evaluări
- Dr. Rabi Dhakal 1 Year MD Resident Department of PediatricDocument29 paginiDr. Rabi Dhakal 1 Year MD Resident Department of PediatricRabi Dhakal100% (1)
- Complement SystemDocument21 paginiComplement SystemEl FatihÎncă nu există evaluări
- Leptospirosis DifferentialDocument4 paginiLeptospirosis DifferentialPatrick DeeÎncă nu există evaluări
- GI Board ReviewDocument176 paginiGI Board Reviewjosh hagsÎncă nu există evaluări
- Pediatric Department Faculty of MedicineDocument100 paginiPediatric Department Faculty of MedicineIrfanÎncă nu există evaluări
- Man Meets Microbes: An Introduction to Medical MicrobiologyDe la EverandMan Meets Microbes: An Introduction to Medical MicrobiologyÎncă nu există evaluări
- ALLERGOLOGY Removals Review by Alec Maquiling: Aureus, E. Coli, C. Difficile), Toxins (ScombroidDocument2 paginiALLERGOLOGY Removals Review by Alec Maquiling: Aureus, E. Coli, C. Difficile), Toxins (ScombroidAlec MaquilingÎncă nu există evaluări
- PericarditisDocument29 paginiPericarditisPavin KumarÎncă nu există evaluări
- Jaundice, (Hyperbilirubinemia) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandJaundice, (Hyperbilirubinemia) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsEvaluare: 5 din 5 stele5/5 (1)
- Anemia of PrematurityDocument14 paginiAnemia of PrematurityMariel HuamancayoÎncă nu există evaluări
- Kernicterus, (Bilirubin Encephalopathy) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandKernicterus, (Bilirubin Encephalopathy) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Anaerobic Infections in HumansDe la EverandAnaerobic Infections in HumansSydney FinegoldEvaluare: 5 din 5 stele5/5 (1)
- Glycogen Storage Disorders PDFDocument4 paginiGlycogen Storage Disorders PDFAHMEDÎncă nu există evaluări
- It 2 - Signs and Symptoms of Git DisordersDocument54 paginiIt 2 - Signs and Symptoms of Git Disorderspikaanisa100% (9)
- Leukaemoid Reaction Lecture by DRDocument35 paginiLeukaemoid Reaction Lecture by DRapi-273068056100% (1)
- Abdominal Pain PDFDocument23 paginiAbdominal Pain PDFSahil DhamijaÎncă nu există evaluări
- Approach To The Child With Anemia - UpToDateDocument41 paginiApproach To The Child With Anemia - UpToDateDaniel Enrique CardenasÎncă nu există evaluări
- Abnormal CBC - PresentationDocument23 paginiAbnormal CBC - PresentationMateen ShukriÎncă nu există evaluări
- Renal DisordersDocument77 paginiRenal Disorderslorelee_espaldon100% (1)
- VOD - SOS in HSCTDocument25 paginiVOD - SOS in HSCTKim-Thinh Nguyen ThiÎncă nu există evaluări
- Hereditary SpherocytosisDocument16 paginiHereditary Spherocytosisrizi2008Încă nu există evaluări
- Optimal Life: Essentials of AsthmaDe la EverandOptimal Life: Essentials of AsthmaÎncă nu există evaluări
- Patho SlidesDocument46 paginiPatho Slidesapi-400411160Încă nu există evaluări
- Non Viral HepatitisDocument40 paginiNon Viral Hepatitisostaz2000100% (1)
- 1.04 Pediatric NutritionDocument6 pagini1.04 Pediatric NutritionJoher Bolante Mendez Jr.Încă nu există evaluări
- Urinalysis ReportDocument88 paginiUrinalysis Reportqwerty masterÎncă nu există evaluări
- VDRL Test and Its InterpretationDocument11 paginiVDRL Test and Its InterpretationSauZen SalaZarÎncă nu există evaluări
- TetanusDocument102 paginiTetanusMo Oo MooÎncă nu există evaluări
- Urinary Tract Infection in Childhood and Its Relevance to Disease in Adult LifeDe la EverandUrinary Tract Infection in Childhood and Its Relevance to Disease in Adult LifeEvaluare: 2 din 5 stele2/5 (2)
- Advances in Pathobiology and Management of Paget’s Disease of BoneDe la EverandAdvances in Pathobiology and Management of Paget’s Disease of BoneSakamuri V. ReddyÎncă nu există evaluări
- Approach To Cyanotic Heart Disease Christopher Cheung Santokh Dhillon PDFDocument13 paginiApproach To Cyanotic Heart Disease Christopher Cheung Santokh Dhillon PDFsuckeydluffyÎncă nu există evaluări
- Approach To Abdominal Masses in ChildrenDocument36 paginiApproach To Abdominal Masses in ChildrenMia Lesaca-Medina100% (3)
- Adnexal MassDocument28 paginiAdnexal MassJuan P. RuedaÎncă nu există evaluări
- Pet-to-Man Travelling Staphylococci: A World in ProgressDe la EverandPet-to-Man Travelling Staphylococci: A World in ProgressVincenzo SaviniÎncă nu există evaluări
- MCQ QuestionsDocument2 paginiMCQ QuestionsShriyans JainÎncă nu există evaluări
- Amniotic Fluid: Group 5Document29 paginiAmniotic Fluid: Group 5Francis ValdezÎncă nu există evaluări
- Medical Management of Children With Down SyndromeDocument8 paginiMedical Management of Children With Down SyndromeMariana OrozcoÎncă nu există evaluări
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Clinical Approach To Neonatal JaundiceDocument17 paginiClinical Approach To Neonatal JaundiceSabera KapasiÎncă nu există evaluări
- Tuberculosis in Infancy and ChildhoodDocument8 paginiTuberculosis in Infancy and ChildhoodsamioÎncă nu există evaluări
- Rheumatic Heart Disease AustrliaDocument63 paginiRheumatic Heart Disease AustrliaMuhammad Reza100% (2)
- Pediatrics SamplexDocument6 paginiPediatrics SamplexThea SansonÎncă nu există evaluări
- AFP Orientation Presentation 2022Document33 paginiAFP Orientation Presentation 2022thqhospital pasrurÎncă nu există evaluări
- Therapeutically Administered Ribonucleoside Analogue Mk-4482/Eidd-2801 Blocks Sars-Cov-2 Transmission in FerretsDocument15 paginiTherapeutically Administered Ribonucleoside Analogue Mk-4482/Eidd-2801 Blocks Sars-Cov-2 Transmission in FerretsCarlosgustavo SaavedrarubioÎncă nu există evaluări
- COVID-19: Dr. Moe Yee Soe Assistant Lecturer Department of Microbiology UM1Document42 paginiCOVID-19: Dr. Moe Yee Soe Assistant Lecturer Department of Microbiology UM1Naing Lin SoeÎncă nu există evaluări
- Daftar Pustaka Bab 1Document5 paginiDaftar Pustaka Bab 1Mahendra Pee WeeÎncă nu există evaluări
- A Case of Primary Myxoid Liposarcoma of The Heart Masquerading As Massive Pericardial Effusion - A Case ReportDocument5 paginiA Case of Primary Myxoid Liposarcoma of The Heart Masquerading As Massive Pericardial Effusion - A Case ReportEditor ERWEJÎncă nu există evaluări
- SARA Alert Product FS 6-23-2020Document2 paginiSARA Alert Product FS 6-23-2020NEWS CENTER MaineÎncă nu există evaluări
- 4 CapDocument11 pagini4 Capshanfiza_92Încă nu există evaluări
- CD Respi 30 ADocument3 paginiCD Respi 30 ANae OrdanozoÎncă nu există evaluări
- Altered Sensorium and Care of Unconscious PatientsDocument17 paginiAltered Sensorium and Care of Unconscious PatientsChhabilal BastolaÎncă nu există evaluări
- ProtozoaDocument2 paginiProtozoaBongTizonDiazÎncă nu există evaluări
- History Form - Ahmad Alalmai 2Document2 paginiHistory Form - Ahmad Alalmai 2heydydÎncă nu există evaluări
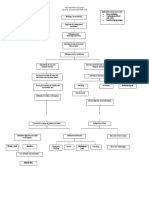
- PathophysiologyDocument3 paginiPathophysiologyKita kita100% (1)
- A Case of Hodgkin Lymphoma Presenting As Nephrotic SyndromeDocument6 paginiA Case of Hodgkin Lymphoma Presenting As Nephrotic SyndromeIJAR JOURNALÎncă nu există evaluări
- 2.a FOOD AND WATERBORNE DISEASES PREVENTION AND CONTROL PROGRAMDocument28 pagini2.a FOOD AND WATERBORNE DISEASES PREVENTION AND CONTROL PROGRAMKieth SeresulaÎncă nu există evaluări
- Hiv Persuasion SpeechDocument2 paginiHiv Persuasion SpeechMaxine De CastroÎncă nu există evaluări
- PP Grade 7 Health JavelinaDocument22 paginiPP Grade 7 Health JavelinaTerry Jane JavelinaÎncă nu există evaluări
- NCP 2 VertigoDocument2 paginiNCP 2 VertigobananakyuÎncă nu există evaluări
- Allergic Conjunctivitis JournalDocument15 paginiAllergic Conjunctivitis JournalSisiliaElfaniPebiantiaÎncă nu există evaluări
- Thinking Skills and Problem Solving Oum Jan 2020Document15 paginiThinking Skills and Problem Solving Oum Jan 2020Shoba ManoharanÎncă nu există evaluări
- Chapter 1Document18 paginiChapter 1Mehar IndiÎncă nu există evaluări
- Initial Antimicrobial Management of Sepsis: Review Open AccessDocument11 paginiInitial Antimicrobial Management of Sepsis: Review Open AccessblanquishemÎncă nu există evaluări
- (PSYCH3) 5.4 The Person With Chronic Mental IllnessDocument3 pagini(PSYCH3) 5.4 The Person With Chronic Mental IllnessDrina PaglinawanÎncă nu există evaluări
- Cyndy Trimm Healing PrayerDocument5 paginiCyndy Trimm Healing Prayermazzagra100% (3)
- SBP - Tushar Kanti Debnath - 20810066Document17 paginiSBP - Tushar Kanti Debnath - 20810066PRANJAL KUMARÎncă nu există evaluări
- Xenex Effectiveness Summary Studies PDFDocument4 paginiXenex Effectiveness Summary Studies PDFREDENLAKE LTDÎncă nu există evaluări
- Terminologi Rambut, Kuku-1Document16 paginiTerminologi Rambut, Kuku-1AuliaÎncă nu există evaluări
- 1 - Concept of Communicble Diseases - 25012013Document107 pagini1 - Concept of Communicble Diseases - 25012013Farhan KabirÎncă nu există evaluări
- Viral HepatitisDocument40 paginiViral Hepatitisinvisibleyetinvincible100% (4)
- q3 Mod2 Activity SheetsDocument2 paginiq3 Mod2 Activity SheetsainsleyÎncă nu există evaluări
- SURGERY Breast DiseasesDocument25 paginiSURGERY Breast DiseasesBiplav SinghÎncă nu există evaluări