S-ar putea să vă placă și
- Frozen ShoulderDocument18 paginiFrozen Shoulderhemnath rajendranÎncă nu există evaluări
- Dr. Mustafa Alshehabat's Guide to Heart Failure Definitions, Causes, Symptoms and TreatmentsDocument20 paginiDr. Mustafa Alshehabat's Guide to Heart Failure Definitions, Causes, Symptoms and TreatmentshuzaifahjusohÎncă nu există evaluări
- Cardiac Stress TestingDocument24 paginiCardiac Stress TestingRhoda Dela Torre ContrerasÎncă nu există evaluări
- Types and Management of Valvular Heart DiseaseDocument60 paginiTypes and Management of Valvular Heart DiseaseIntan Kumalasari RambeÎncă nu există evaluări
- Advanced Cardiac ProcedureDocument9 paginiAdvanced Cardiac ProcedureSachin DwivediÎncă nu există evaluări
- Cardiomyopathy: Leonard Shaju Joisy AloorDocument34 paginiCardiomyopathy: Leonard Shaju Joisy AloorJoisy AloorÎncă nu există evaluări
- Approach to Chest Pain, Edema and PalpitationsDocument18 paginiApproach to Chest Pain, Edema and PalpitationsNoreenÎncă nu există evaluări
- Doppler UltrasoundDocument3 paginiDoppler UltrasoundDrShagufta IqbalÎncă nu există evaluări
- Ventricular Fibrillation/ Pulseless Ventricular Tachycardia AlgorithmDocument2 paginiVentricular Fibrillation/ Pulseless Ventricular Tachycardia AlgorithmsafasayedÎncă nu există evaluări
- Tress Test: The Gale Encyclopedia of MedicineDocument7 paginiTress Test: The Gale Encyclopedia of MedicineSalsabilla KimikoÎncă nu există evaluări
- M1167 HMMWV Expanded Capacity TOW Missile CarrierDocument2 paginiM1167 HMMWV Expanded Capacity TOW Missile CarrierSergeant_2011100% (1)
- Management Acute StrokeDocument108 paginiManagement Acute StrokeratuhamimÎncă nu există evaluări
- Exercise Testing: Acc/Aha Practice Guidelines GibbonsDocument47 paginiExercise Testing: Acc/Aha Practice Guidelines GibbonsviKиҼswAяAи LiиGaMÎncă nu există evaluări
- Valvular Heart Disease To TW FinalDocument13 paginiValvular Heart Disease To TW FinalMohammed ElSayedÎncă nu există evaluări
- Ventricular ArrhythmiasDocument33 paginiVentricular ArrhythmiasSamantha DeshapriyaÎncă nu există evaluări
- Emergency Drugs KathDocument29 paginiEmergency Drugs Kathmajin655Încă nu există evaluări
- Performing Exercise Treadmill TestingDocument60 paginiPerforming Exercise Treadmill Testingvera_yulia98Încă nu există evaluări
- Hemiplegia Rehabilitation TechniquesDocument11 paginiHemiplegia Rehabilitation TechniquesFares EL DeenÎncă nu există evaluări
- PERICARDITISDocument11 paginiPERICARDITISsalman hÎncă nu există evaluări
- Everything You Need to Know About DiabetesDocument39 paginiEverything You Need to Know About DiabetesSubramaniam RamanÎncă nu există evaluări
- Exercise Stress Testing GuidelinesDocument15 paginiExercise Stress Testing GuidelinesStevco Donev MakedonskiÎncă nu există evaluări
- Cardiovascular Disorders: BY: Maximin A. Pomperada, RN, MANDocument65 paginiCardiovascular Disorders: BY: Maximin A. Pomperada, RN, MANRellie Castro100% (1)
- Early Pregnancy Bleeding Causes and TypesDocument51 paginiEarly Pregnancy Bleeding Causes and TypesMesk Banat100% (2)
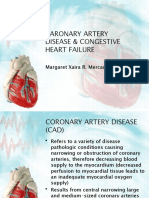
- Caronary Artery Disease & Congestive Heart Failure: Margaret Xaira R. Mercado RNDocument32 paginiCaronary Artery Disease & Congestive Heart Failure: Margaret Xaira R. Mercado RNMargaret Xaira Rubio MercadoÎncă nu există evaluări
- Olympic Skier's Asthma TreatmentDocument41 paginiOlympic Skier's Asthma TreatmentLeong Zhee ChuanÎncă nu există evaluări
- IV Fluid Types and UsesDocument6 paginiIV Fluid Types and UsesKiara Denise TamayoÎncă nu există evaluări
- #6 Copd 11 PDFDocument11 pagini#6 Copd 11 PDFOmar BasimÎncă nu există evaluări
- Chest Pain: Sumit Bose, MD PGY-3Document55 paginiChest Pain: Sumit Bose, MD PGY-3Irfan100% (1)
- Interpreting The Exercise Test ResultsDocument26 paginiInterpreting The Exercise Test ResultssalsabilaÎncă nu există evaluări
- Holter Monitor: 'Ambulatory Electrocardiography Device''Document22 paginiHolter Monitor: 'Ambulatory Electrocardiography Device''Rachel PeredaÎncă nu există evaluări
- Interpretation of Clinical Biochemical TestsDocument24 paginiInterpretation of Clinical Biochemical TestsaddwrÎncă nu există evaluări
- Local Stress CheckDocument7 paginiLocal Stress Checkprabhakaran.cÎncă nu există evaluări
- Sis SabaDocument295 paginiSis Sabaghoongru67% (3)
- BOILS (Furuncle) : Shashank JoshiDocument10 paginiBOILS (Furuncle) : Shashank JoshiKapil LakhwaraÎncă nu există evaluări
- Malabsorption: Causes, Symptoms, and TreatmentDocument75 paginiMalabsorption: Causes, Symptoms, and TreatmentLaith Al TamimiÎncă nu există evaluări
- Fluid and Electrolytes Replacement TherapyDocument49 paginiFluid and Electrolytes Replacement TherapyMarife MartinÎncă nu există evaluări
- Basic Respiratory Mechanics: Ventilation, Diffusion, and Gas ExchangeDocument36 paginiBasic Respiratory Mechanics: Ventilation, Diffusion, and Gas ExchangeRizqi Luqmanul HakimÎncă nu există evaluări
- 694+ Illustrated Parts Catalog Revision 3.1 FROM SERIAL TRX01694CDGL11965Document549 pagini694+ Illustrated Parts Catalog Revision 3.1 FROM SERIAL TRX01694CDGL11965Martín Lescano ParedesÎncă nu există evaluări
- Engargoladora de LatasDocument21 paginiEngargoladora de LatasAngel PerezÎncă nu există evaluări
- Nursing Management of Breast DisordersDocument89 paginiNursing Management of Breast DisordersYang TayengÎncă nu există evaluări
- St. Luke's Echocardiogram Patient GuideDocument2 paginiSt. Luke's Echocardiogram Patient Guideteju13aÎncă nu există evaluări
- Electrocardiogram (EKG or ECG)Document12 paginiElectrocardiogram (EKG or ECG)श्रीकृष्ण हेङ्गजूÎncă nu există evaluări
- HypertensionDocument21 paginiHypertensionM RaisÎncă nu există evaluări
- Chest Injuries GuideDocument19 paginiChest Injuries GuideAbdi Kumala100% (1)
- Range of Motion ExercisesDocument13 paginiRange of Motion Exercisesmoira77Încă nu există evaluări
- Introduction Definition: Types of PacemakersDocument8 paginiIntroduction Definition: Types of PacemakersPrasann RoyÎncă nu există evaluări
- Treadmill Test: Khairul Nizam Abdul Rahman 4262143008Document12 paginiTreadmill Test: Khairul Nizam Abdul Rahman 4262143008Dea Amelia YolandaÎncă nu există evaluări
- Bells Palsy DorisDocument37 paginiBells Palsy DoristheychemÎncă nu există evaluări
- Posterior Urethral ValveDocument6 paginiPosterior Urethral ValveMustafa AadanÎncă nu există evaluări
- P Ap SmearDocument4 paginiP Ap SmearKinjal VasavaÎncă nu există evaluări
- Antituberculous Therapy in Special SituationsDocument8 paginiAntituberculous Therapy in Special SituationsMobeen Raza100% (1)
- Treadmill Test: Khairul Nizam Abdul Rahman 4262143008Document12 paginiTreadmill Test: Khairul Nizam Abdul Rahman 4262143008Dea Amelia YolandaÎncă nu există evaluări
- Understanding Low Blood PressureDocument6 paginiUnderstanding Low Blood PressureRajeev Nechiyil100% (1)
- Gullaine-Barré SyndromeDocument13 paginiGullaine-Barré SyndromeOnieBoy CurayagÎncă nu există evaluări
- Lower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocument95 paginiLower Respiratory Tract Infections: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingRI NAÎncă nu există evaluări
- BreastDocument2 paginiBreastPretty UÎncă nu există evaluări
- A Guide To ECG Reporting For Year 3 Medical StudentsDocument2 paginiA Guide To ECG Reporting For Year 3 Medical StudentscsngiuÎncă nu există evaluări
- InhalDocument33 paginiInhallupeÎncă nu există evaluări
- Arterial Blood PressureDocument21 paginiArterial Blood PressureMaham SaleemÎncă nu există evaluări
- Holter MonitoringDocument19 paginiHolter Monitoringomotola Ayobundle-oyewo MA206100% (1)
- Test Report Gupta DiagnosisDocument17 paginiTest Report Gupta Diagnosisdrblgupta1973100% (1)
- AnginaDocument12 paginiAnginaDr-Sanjay SinghaniaÎncă nu există evaluări
- Intravenous Fluid Therapy in Adults in The HospitalDocument28 paginiIntravenous Fluid Therapy in Adults in The Hospitalushapadminivadivelswamy100% (2)
- Poisoning in ChildrenDocument11 paginiPoisoning in ChildrenAndriana HalfienÎncă nu există evaluări
- Echocardiogram MayoDocument4 paginiEchocardiogram MayoMarta KitaÎncă nu există evaluări
- Lapsus LSKDocument22 paginiLapsus LSKYaumilKhalidaÎncă nu există evaluări
- Jurnal Forensik ReprodusibilitasDocument3 paginiJurnal Forensik ReprodusibilitasYaumilKhalidaÎncă nu există evaluări
- Update Keratitis CompressedDocument13 paginiUpdate Keratitis CompressedYaumilKhalidaÎncă nu există evaluări
- SOAP CardioDocument1 paginăSOAP CardioYaumilKhalidaÎncă nu există evaluări
- Am J Clin Nutr 2008 O'Donnell 1388 95Document8 paginiAm J Clin Nutr 2008 O'Donnell 1388 95YaumilKhalidaÎncă nu există evaluări
- CSS Sox2Document18 paginiCSS Sox2YaumilKhalidaÎncă nu există evaluări
- Clinical Practice Guideline: Tonsillitis I. Diagnostics and Nonsurgical ManagementDocument15 paginiClinical Practice Guideline: Tonsillitis I. Diagnostics and Nonsurgical ManagementTuti Nursyah PutriÎncă nu există evaluări
- EAU Guidelines Renal Cell Carcinoma 2016Document62 paginiEAU Guidelines Renal Cell Carcinoma 2016SandroLaoÎncă nu există evaluări
- 835 3343 1 PBDocument7 pagini835 3343 1 PBYaumilKhalidaÎncă nu există evaluări
- Impact of Imposed Exercise On Energy Intake in Children at Risk For OverweightDocument9 paginiImpact of Imposed Exercise On Energy Intake in Children at Risk For OverweightYaumilKhalidaÎncă nu există evaluări
- Major Muscles of the Hip and LegDocument5 paginiMajor Muscles of the Hip and LegYaumilKhalidaÎncă nu există evaluări
- Health-Promotion and Disease-Prevention Behaviors of Primary-Care PractitionersDocument9 paginiHealth-Promotion and Disease-Prevention Behaviors of Primary-Care PractitionersYaumilKhalidaÎncă nu există evaluări
- Emotional and Physiologic Elements of Death and DyingDocument17 paginiEmotional and Physiologic Elements of Death and DyinghengkihanggaraÎncă nu există evaluări
- English in M TestDocument4 paginiEnglish in M TestNicoleta NovosutchiÎncă nu există evaluări
- Daftar Game HDDocument8 paginiDaftar Game HDIkhwan Sya'bani SalimÎncă nu există evaluări
- Results For Engine Code - DV6DTED - Meat&DoriaDocument3 paginiResults For Engine Code - DV6DTED - Meat&Doriaبيرش امينÎncă nu există evaluări
- Nair Question Bank Participants of Grade A Foundation Course CommercialDocument8 paginiNair Question Bank Participants of Grade A Foundation Course CommercialSudheer ChauhanÎncă nu există evaluări
- Jason Behrendorff: Personal Information Full Name BornDocument2 paginiJason Behrendorff: Personal Information Full Name BornRashid AnwerÎncă nu există evaluări
- Name: Date: - Year/Section:: Task 1: PAR-Q and YOU Questionnaire (Prior To The Activity Test)Document3 paginiName: Date: - Year/Section:: Task 1: PAR-Q and YOU Questionnaire (Prior To The Activity Test)Angela Louise Smiths0% (1)
- 359566-2linde 11.5 Meter R16 PDFDocument1 pagină359566-2linde 11.5 Meter R16 PDFASIFÎncă nu există evaluări
- Afl Fact SheetDocument1 paginăAfl Fact Sheetapi-257609033Încă nu există evaluări
- Verbs 2Document2 paginiVerbs 2bruceÎncă nu există evaluări
- Soal+PAT+B ING+Kelas+8+K13++-+www Kherysuryawan IdDocument8 paginiSoal+PAT+B ING+Kelas+8+K13++-+www Kherysuryawan Idwahyu prasetiyoÎncă nu există evaluări
- CFORCE 450 - 520 BrochureDocument14 paginiCFORCE 450 - 520 BrochureRat MarianÎncă nu există evaluări
- Online Review AnswersDocument15 paginiOnline Review AnswersdebshistoryfairÎncă nu există evaluări
- WorkoutplnDocument2 paginiWorkoutplnJaneth FrenchÎncă nu există evaluări
- EzyMath Percentages WorksheetDocument2 paginiEzyMath Percentages WorksheetOzÎncă nu există evaluări
- Disegno - Nuova - Torre MilotDocument1 paginăDisegno - Nuova - Torre MilotRejnald ZyfiÎncă nu există evaluări
- Warscroll: Chameleon SkinksDocument1 paginăWarscroll: Chameleon SkinksMax WyattÎncă nu există evaluări
- Statement of ClaimDocument17 paginiStatement of ClaimUbysseyNewsÎncă nu există evaluări
- Maxon GS 16 ADocument1 paginăMaxon GS 16 AElectromateÎncă nu există evaluări
- Change LogDocument13 paginiChange LogAndreson PimentelÎncă nu există evaluări
- Fast Character - D&D Character Maker - Saytr - Faun Sorcerer 1Document1 paginăFast Character - D&D Character Maker - Saytr - Faun Sorcerer 1vel ledaÎncă nu există evaluări
- Qdoc - Tips Tiger Tracks 5 Test Unit 1Document10 paginiQdoc - Tips Tiger Tracks 5 Test Unit 1esperanza100% (1)
- Nuevos ModsDocument2 paginiNuevos ModssergioÎncă nu există evaluări
- Dime UploadsDocument14 paginiDime UploadsGianmaria RizzardiÎncă nu există evaluări
- The Long JumpDocument7 paginiThe Long JumpjadahÎncă nu există evaluări