S-ar putea să vă placă și
- Ischemic Heart DiseaseDocument5 paginiIschemic Heart DiseaseBert DivinagraciaÎncă nu există evaluări
- Ischemic Heart DiseaseDocument13 paginiIschemic Heart Diseasegyspsunshine girlÎncă nu există evaluări
- AtherosclerosisDocument56 paginiAtherosclerosisJohn Matley Caampued100% (8)
- Congestive Heart FailureDocument14 paginiCongestive Heart FailureBella Trix PagdangananÎncă nu există evaluări
- AsthmaDocument59 paginiAsthmaGulzar Ahmad RawnÎncă nu există evaluări
- Ischemic Heart DiseaseDocument116 paginiIschemic Heart Diseasedrmsupriya09115983% (6)
- Ischemic Heart Disease PWDocument13 paginiIschemic Heart Disease PWEunica RamosÎncă nu există evaluări
- MF3 - Ischemic Heart DiseaseDocument28 paginiMF3 - Ischemic Heart DiseaseAnnbe BarteÎncă nu există evaluări
- Bachelor of Nursing Science With HonoursDocument17 paginiBachelor of Nursing Science With HonoursMaryam HasanahÎncă nu există evaluări
- Pathophysiology of Heart FailureDocument1 paginăPathophysiology of Heart Failureiz11Încă nu există evaluări
- Chronic Obstructive Pulmonary Disease (COPD) : Sultan Chaudhry Benny Dua Eric WongDocument7 paginiChronic Obstructive Pulmonary Disease (COPD) : Sultan Chaudhry Benny Dua Eric Wongjamil aldasriÎncă nu există evaluări
- Heart Attack Risk Factors and DiagnosisDocument67 paginiHeart Attack Risk Factors and DiagnosisJoshua Pascasio100% (1)
- Atherosclerosis PathophysiologyDocument11 paginiAtherosclerosis PathophysiologyCandice ChengÎncă nu există evaluări
- Heart FailureDocument10 paginiHeart Failureurmila prajapatiÎncă nu există evaluări
- Myocardial InfarctionDocument40 paginiMyocardial InfarctionHIRANGER100% (3)
- Atherosclerosis 2 2017 (Modified)Document64 paginiAtherosclerosis 2 2017 (Modified)Remo B AbyÎncă nu există evaluări
- Pathophysiology of AtherosclerosisDocument27 paginiPathophysiology of AtherosclerosisAmira Paguyo QuilapioÎncă nu există evaluări
- Acute Myocardial InfarctionDocument14 paginiAcute Myocardial InfarctionJardee DatsimaÎncă nu există evaluări
- Myocardial InfarctionDocument15 paginiMyocardial InfarctionameerÎncă nu există evaluări
- Nephrotic Syndrome PathophysiologyDocument1 paginăNephrotic Syndrome PathophysiologyKrisianne Mae Lorenzo FranciscoÎncă nu există evaluări
- CONGESTIVE HEART FAILURE NURSING CAREDocument33 paginiCONGESTIVE HEART FAILURE NURSING CARENikki M. ArapolÎncă nu există evaluări
- Pulmonary EmbolismDocument14 paginiPulmonary EmbolismAngel Naypes ReyesÎncă nu există evaluări
- Pathophysiology Infective EarditisDocument3 paginiPathophysiology Infective EarditisDanielJosephLim50% (2)
- Pathophysiology of Atherosclerosis, Thrombosis and EmbolismDocument4 paginiPathophysiology of Atherosclerosis, Thrombosis and EmbolismKeshant Samaroo100% (1)
- Pneumonia PresentationDocument20 paginiPneumonia PresentationsetanpikulanÎncă nu există evaluări
- Respiratory EmergenciesDocument30 paginiRespiratory EmergenciesNovriefta NugrahaÎncă nu există evaluări
- Pulmonary Embolism Guide: Causes, Symptoms & DiagnosisDocument60 paginiPulmonary Embolism Guide: Causes, Symptoms & DiagnosisRafika RaraÎncă nu există evaluări
- Bronchial AsthmaDocument43 paginiBronchial AsthmaAmar BimavarapuÎncă nu există evaluări
- Pathology of The Lung: Djumadi AchmadDocument26 paginiPathology of The Lung: Djumadi AchmadVivi DeviyanaÎncă nu există evaluări
- LA Myxoma Case PresentationDocument34 paginiLA Myxoma Case PresentationWiwik Puji LestariÎncă nu există evaluări
- Coronary Artery Disease: Causes, Risks, and PreventionDocument80 paginiCoronary Artery Disease: Causes, Risks, and Preventionamelia pratiwiÎncă nu există evaluări
- Ischemic Heart DiseaseDocument8 paginiIschemic Heart DiseaseNina Natalia Bautista100% (1)
- Ischemic StrokeDocument49 paginiIschemic StrokeMirna Ayu Permata SariÎncă nu există evaluări
- Myocardial InfarctionDocument47 paginiMyocardial Infarctionsanjesh1100% (2)
- Acute Rheumatic Fever - Clinical Manifestations and Diagnosis - UpToDateDocument15 paginiAcute Rheumatic Fever - Clinical Manifestations and Diagnosis - UpToDateDannyGutierrezÎncă nu există evaluări
- Pathophysiology of ArrhythmiasDocument15 paginiPathophysiology of ArrhythmiasJonathan MontecilloÎncă nu există evaluări
- Renal FailureDocument56 paginiRenal FailureKoRnflakes100% (2)
- EPIGLOTTITISDocument9 paginiEPIGLOTTITISanon_944507650Încă nu există evaluări
- Chronic Renal FailureDocument14 paginiChronic Renal FailureyazzzÎncă nu există evaluări
- Acute Myocardial InfarctionDocument2 paginiAcute Myocardial InfarctionhailleyannÎncă nu există evaluări
- COPD Treatment by StageDocument35 paginiCOPD Treatment by StageNurhidayahÎncă nu există evaluări
- Portal HypertensionDocument65 paginiPortal HypertensionVenu MadhavÎncă nu există evaluări
- Acute Glomerulonephritis Case StudyDocument6 paginiAcute Glomerulonephritis Case StudyjakerzÎncă nu există evaluări
- Ischemic Heart DiseaseDocument39 paginiIschemic Heart DiseaserahulbafnaeÎncă nu există evaluări
- Congestive Heart Failure PathophysiologyDocument16 paginiCongestive Heart Failure PathophysiologyDale LaurenteÎncă nu există evaluări
- Aneurysm Final (Bentals Procedure)Document55 paginiAneurysm Final (Bentals Procedure)tejuteju067100% (1)
- Asthma: Nurse AvenueDocument13 paginiAsthma: Nurse AvenueWindi Lameck MarwaÎncă nu există evaluări
- Predisposing and precipitating factors leading to ESRD, DM, atherosclerosis, and pneumoniaDocument11 paginiPredisposing and precipitating factors leading to ESRD, DM, atherosclerosis, and pneumoniaJonathan CuaÎncă nu există evaluări
- General Pathophysiology: Predisposing Factors: Precipitating FactorsDocument2 paginiGeneral Pathophysiology: Predisposing Factors: Precipitating FactorsIrish Nicole DCÎncă nu există evaluări
- Heart Failure (Recovered)Document43 paginiHeart Failure (Recovered)Binal Joshi100% (1)
- Acute Coronary Syndromes-PresentationDocument86 paginiAcute Coronary Syndromes-Presentationpatange jayaprakash rahul100% (4)
- Pulmonary EdemaDocument59 paginiPulmonary EdemamaibejoseÎncă nu există evaluări
- Bronchial AsthmaDocument54 paginiBronchial AsthmaSehar162100% (2)
- Nursing Management of Patient with Ovarian CancerDocument7 paginiNursing Management of Patient with Ovarian CancerTerrena Lyn BlackmanÎncă nu există evaluări
- Case Study PPT Patho NLNGDocument36 paginiCase Study PPT Patho NLNGKate ChavezÎncă nu există evaluări
- Causes and Pathophysiology of Congestive Heart Failure (CHFDocument1 paginăCauses and Pathophysiology of Congestive Heart Failure (CHFLance MarquezÎncă nu există evaluări
- Pa Tho Physiology of Diabetes MellitusDocument3 paginiPa Tho Physiology of Diabetes MellitusPong's Teodoro SalvadorÎncă nu există evaluări
- StrokeDocument17 paginiStrokeJo CanensÎncă nu există evaluări
- 5 - Pathology of CADDocument58 pagini5 - Pathology of CADregeti bhargavÎncă nu există evaluări
- Heart Guide 2022Document13 paginiHeart Guide 2022AnuÎncă nu există evaluări
- Calander High Court2017Document3 paginiCalander High Court2017born_321118403Încă nu există evaluări
- Regulations and Curricula for Post Graduate Degree and Diploma Courses in Medical Sciences 2000Document39 paginiRegulations and Curricula for Post Graduate Degree and Diploma Courses in Medical Sciences 2000born_321118403Încă nu există evaluări
- 2 Nausea Choosing Antiemetics DR Robin LoveDocument31 pagini2 Nausea Choosing Antiemetics DR Robin LoveAndrew Yoshihiro WiryaÎncă nu există evaluări
- August2016 Drug Approvals and ChangesDocument19 paginiAugust2016 Drug Approvals and Changesborn_321118403Încă nu există evaluări
- h1n1 Guidelines Pharmaceutical MNGTDocument32 paginih1n1 Guidelines Pharmaceutical MNGThossamh3Încă nu există evaluări
- WHO Dengue Guidelines 2013Document160 paginiWHO Dengue Guidelines 2013Jason MirasolÎncă nu există evaluări
- 1000 Popular Words in EnglishDocument13 pagini1000 Popular Words in EnglishDaongocÎncă nu există evaluări
- ACS and ECGDocument33 paginiACS and ECGborn_321118403Încă nu există evaluări
- Approach To Locomotor SystemDocument24 paginiApproach To Locomotor Systemborn_321118403Încă nu există evaluări
- ART guidelines for HIV-Infected Adults and AdolescentsDocument122 paginiART guidelines for HIV-Infected Adults and AdolescentsRohitKumarÎncă nu există evaluări
- Premix Analogue VS. Premix Human Insulin Clinical DifferencesDocument36 paginiPremix Analogue VS. Premix Human Insulin Clinical Differencesborn_321118403Încă nu există evaluări
- HIV RecommendationDocument11 paginiHIV Recommendationborn_321118403Încă nu există evaluări
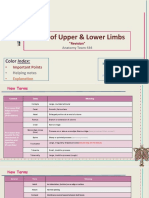
- Bones of Upper and Lower Limbs - RevisionDocument15 paginiBones of Upper and Lower Limbs - RevisionChess Nuts100% (1)
- 2. Atlas of Anatomy. Netter 3. An Atlas Of Surgical Anatomy Masquelet.pdf 4. Anatomie Sрringer.pdf 5. Anatomy Coloring Book Benjamin Cummings PDFDocument2 pagini2. Atlas of Anatomy. Netter 3. An Atlas Of Surgical Anatomy Masquelet.pdf 4. Anatomie Sрringer.pdf 5. Anatomy Coloring Book Benjamin Cummings PDFmrmarcoguimaÎncă nu există evaluări
- 10,11-Arterial Blood Pressure & Its Regulation Team441Document51 pagini10,11-Arterial Blood Pressure & Its Regulation Team441saran kÎncă nu există evaluări
- The Nervous System & Our Brain PowerPoint - Krishna ShilDocument21 paginiThe Nervous System & Our Brain PowerPoint - Krishna ShilKrishna ShilÎncă nu există evaluări
- Abdominal Pain Diagnosis and Treatment PlanDocument2 paginiAbdominal Pain Diagnosis and Treatment PlanSandhya Rubens67% (9)
- ALVINA Research-1Document3 paginiALVINA Research-1Alvina MudyandariÎncă nu există evaluări
- Hyoid BoneDocument31 paginiHyoid Bonekhorrami4Încă nu există evaluări
- Reviewer Science For Grade 9 StudentsDocument29 paginiReviewer Science For Grade 9 StudentsevanescentÎncă nu există evaluări
- Chronic Kidney Disease Case StudyDocument49 paginiChronic Kidney Disease Case StudyHope Tome100% (1)
- Parotid Gland Notes AnatomyDocument6 paginiParotid Gland Notes Anatomykingmbbs30Încă nu există evaluări
- Worksheet BiologyDocument2 paginiWorksheet BiologyRidham JainÎncă nu există evaluări
- 107 Rotator Cuff Exercises - Zach CalhoonDocument136 pagini107 Rotator Cuff Exercises - Zach CalhoonSam Gregory100% (2)
- USG of Normal Musculoskeletal StructuresDocument7 paginiUSG of Normal Musculoskeletal StructuresDhisa Zainita HabsariÎncă nu există evaluări
- Scapula Fracture: DR Jaseem ShamsudeenDocument32 paginiScapula Fracture: DR Jaseem ShamsudeenJaseemshams ThottiyilÎncă nu există evaluări
- Article PDF Neeraj Madan Nidhi Kathuria 49Document3 paginiArticle PDF Neeraj Madan Nidhi Kathuria 49evieramawati_4536812Încă nu există evaluări
- Sukshma and Sthula VyayamaDocument1 paginăSukshma and Sthula VyayamaKomal MandeÎncă nu există evaluări
- Sample Patient Initial EvaluationDocument8 paginiSample Patient Initial EvaluationYang TubioÎncă nu există evaluări
- Digestive System Anatomy and Physiology - NurseslabsDocument33 paginiDigestive System Anatomy and Physiology - NurseslabsMari FeÎncă nu există evaluări
- SHS Q2 WK5 M5 Melc2Document20 paginiSHS Q2 WK5 M5 Melc2Ruthsen Navo MagnayeÎncă nu există evaluări
- STOMACHDocument20 paginiSTOMACHChoudhary FahadÎncă nu există evaluări
- 1402AHS Prac Manual - 2023 - FINALDocument200 pagini1402AHS Prac Manual - 2023 - FINALRuan BritsÎncă nu există evaluări
- 10 The Nervous System 2Document6 pagini10 The Nervous System 2Cristina AdolfoÎncă nu există evaluări
- 1513968174.valsotic BearvDocument6 pagini1513968174.valsotic BearvSentinel Playz TMÎncă nu există evaluări
- 7D Hifu HF700Document49 pagini7D Hifu HF700Jonathan AvilesÎncă nu există evaluări
- CSFDocument40 paginiCSFDrNaveen Singh Rajpurohit KaduÎncă nu există evaluări
- Surgical Anatomy of The Neck: Cervical Fascia: Head & Neck Surgery CourseDocument10 paginiSurgical Anatomy of The Neck: Cervical Fascia: Head & Neck Surgery CourseΑΘΑΝΑΣΙΟΣ ΚΟΥΤΟΥΚΤΣΗΣÎncă nu există evaluări
- Biomechanics of Head and NeckDocument14 paginiBiomechanics of Head and NeckMann SabahÎncă nu există evaluări
- 1.1 Human Breathing MechanismDocument2 pagini1.1 Human Breathing Mechanismieya_yÎncă nu există evaluări
- Lab Exercise No. 5: X-Ray Identification Activity: Name: Rocel Marie D. Lopez Section: BSN 1105Document11 paginiLab Exercise No. 5: X-Ray Identification Activity: Name: Rocel Marie D. Lopez Section: BSN 1105Rocel Marie Lopez100% (1)
- Surya Namaskar ExplanationDocument17 paginiSurya Namaskar Explanationnaresh08Încă nu există evaluări