S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Biology Project Report: Submitted To: Submitted byDocument19 paginiBiology Project Report: Submitted To: Submitted byNIKHIL SINGH89% (28)
- The Encyclopedia of Work-Related Ilnesses, Injuries, and Health IssuesDocument379 paginiThe Encyclopedia of Work-Related Ilnesses, Injuries, and Health IssuesRoxana VaratuceanuÎncă nu există evaluări
- Third Quarter Science 10 - BiologyDocument91 paginiThird Quarter Science 10 - BiologyApple ArellanoÎncă nu există evaluări
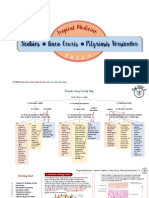
- Scabies Tinea Cruris Pityriasis Versicolor: Semangat!Document11 paginiScabies Tinea Cruris Pityriasis Versicolor: Semangat!Fitriah Nur SyamiatiÎncă nu există evaluări
- Insulin, Regular (Humulin R)Document1 paginăInsulin, Regular (Humulin R)EÎncă nu există evaluări
- @ (White Paper Cut-Off) QUS 0202 FinalDocument13 pagini@ (White Paper Cut-Off) QUS 0202 FinalHajjab AnasÎncă nu există evaluări
- Safety Data Sheet: Section 1. Chemical Product and Company IdentificationDocument17 paginiSafety Data Sheet: Section 1. Chemical Product and Company IdentificationEngr Qaisar NazeerÎncă nu există evaluări
- HSV1 HSV2 R-Gene & VZV R-GeneDocument2 paginiHSV1 HSV2 R-Gene & VZV R-GeneSachinÎncă nu există evaluări
- Table 1 Classification and Staging Systems For AKIDocument1 paginăTable 1 Classification and Staging Systems For AKIAnityo NugrohoÎncă nu există evaluări
- Dr. Naitik D Trivedi & Dr. Upama N. Trivedi: Pharmacology and Toxicology PracticalDocument2 paginiDr. Naitik D Trivedi & Dr. Upama N. Trivedi: Pharmacology and Toxicology PracticalAnjali RaulÎncă nu există evaluări
- LoadVoucher AspxDocument4 paginiLoadVoucher AspxEdnalyn CasasÎncă nu există evaluări
- CC.14.01 Pre and Post Operative CareDocument3 paginiCC.14.01 Pre and Post Operative CareKrupaÎncă nu există evaluări
- Care of Elderly - NCP1Document2 paginiCare of Elderly - NCP1ROGEN KATE AZARCONÎncă nu există evaluări
- Structure of The NailDocument33 paginiStructure of The NailYen100% (1)
- Sedatives, Hypnotics & Anxiolytics (Antianxiety Drugs) Ms. S.R.DhandeDocument347 paginiSedatives, Hypnotics & Anxiolytics (Antianxiety Drugs) Ms. S.R.DhandeEsha pantÎncă nu există evaluări
- Case Conference Maternal HIV C Maternal Amphetamine Use PDFDocument44 paginiCase Conference Maternal HIV C Maternal Amphetamine Use PDFPloyz NattidaÎncă nu există evaluări
- INTRODUCTIONDocument3 paginiINTRODUCTIONSoumya Suguna TripathyÎncă nu există evaluări
- Dental AuxillaryDocument125 paginiDental AuxillaryAME DENTAL COLLEGE RAICHUR, KARNATAKAÎncă nu există evaluări
- Hypertension NCLEX Quiz Questions: A. I Will Make Sure I Consume Foods High in PotassiumDocument5 paginiHypertension NCLEX Quiz Questions: A. I Will Make Sure I Consume Foods High in PotassiumMelodia Turqueza GandezaÎncă nu există evaluări
- 0 - Hospital Design 2020 PDFDocument3 pagini0 - Hospital Design 2020 PDFPriya DharshiniÎncă nu există evaluări
- Information 13 00059 v2Document18 paginiInformation 13 00059 v2hendranatjÎncă nu există evaluări
- Universal PrecutionsDocument30 paginiUniversal PrecutionsShirmi BamunusingheÎncă nu există evaluări
- Instilling Otic/Ear Drops Procedure RationaleDocument12 paginiInstilling Otic/Ear Drops Procedure RationaleBSN2-F MASINING NA PAGPAPAHAYAGÎncă nu există evaluări
- NCM312 PPT Operating Room NursingDocument132 paginiNCM312 PPT Operating Room NursingNine SoleilÎncă nu există evaluări
- Understanding The Different Routes of Drug AdministrationDocument3 paginiUnderstanding The Different Routes of Drug AdministrationMark Russel Sean LealÎncă nu există evaluări
- Benefits of HijamaDocument3 paginiBenefits of HijamaBateria MeaÎncă nu există evaluări
- Disorders of The Reproductive SystemDocument10 paginiDisorders of The Reproductive SystemRose Kathreen Quintans AuxteroÎncă nu există evaluări
- Mcqs FinalDocument4 paginiMcqs FinalJats_Fru_1741Încă nu există evaluări
- Hemorrhage PathophysiologyDocument3 paginiHemorrhage PathophysiologyJubelle Sipalay0% (1)
- Goiter: What Is The Thyroid Gland?Document2 paginiGoiter: What Is The Thyroid Gland?Julio LeviÎncă nu există evaluări