S-ar putea să vă placă și
- Okana Odu: Jobs, Love, Position at Risk"TITLE"Ellioko Odu: End of Cycle, Family Conflicts, Inheritance" TITLE"Oggunda Odu: Need Guidance, Problem Not Yet SolvedDocument33 paginiOkana Odu: Jobs, Love, Position at Risk"TITLE"Ellioko Odu: End of Cycle, Family Conflicts, Inheritance" TITLE"Oggunda Odu: Need Guidance, Problem Not Yet SolvedJuan MonteroÎncă nu există evaluări
- Copd 2022Document45 paginiCopd 2022Mubassir NisarÎncă nu există evaluări
- Respiratory SystemDocument9 paginiRespiratory Systemtheglobalnursing89% (9)
- Aerosols and the Lung: Clinical and Experimental AspectsDe la EverandAerosols and the Lung: Clinical and Experimental AspectsStewart W. ClarkeÎncă nu există evaluări
- Nursing Care Management - 112Document67 paginiNursing Care Management - 112Ong KarlÎncă nu există evaluări
- Acute Respiratory Failure LectureDocument53 paginiAcute Respiratory Failure Lectureprototypeallhell100% (2)
- Respiratory DisordersDocument18 paginiRespiratory Disordersjdigal100% (4)
- Rare and Interesting Cases in Pulmonary MedicineDe la EverandRare and Interesting Cases in Pulmonary MedicineEvaluare: 4 din 5 stele4/5 (1)
- Clinical PathwayDocument154 paginiClinical Pathwaywirdahaja100% (1)
- Common Nursing AbbreviationsDocument5 paginiCommon Nursing AbbreviationsJeffÎncă nu există evaluări
- Asthma + COPD (Full)Document115 paginiAsthma + COPD (Full)selamsew alemuÎncă nu există evaluări
- Seminar2saliva 160425090015 PDFDocument101 paginiSeminar2saliva 160425090015 PDFYus Arlika Putra WibawaÎncă nu există evaluări
- PNEUMONIA CASE STUDY PRESENTATIONDocument29 paginiPNEUMONIA CASE STUDY PRESENTATIONYamSomandar0% (1)
- Pharmacotherapy For COPD: Prepared ByDocument35 paginiPharmacotherapy For COPD: Prepared ByYogi RavalÎncă nu există evaluări
- Hypothyroidism T3 T4 Triglycerides Clinical ChemistryDocument11 paginiHypothyroidism T3 T4 Triglycerides Clinical ChemistryRitz Bautista Balanay100% (1)
- Gpat - 2018 Question PaperDocument14 paginiGpat - 2018 Question PaperKamalendu PandeyÎncă nu există evaluări
- Respiratory FailureDocument52 paginiRespiratory FailureMohammad_Islam87100% (8)
- Med Surg I Exam 1 ReviewDocument8 paginiMed Surg I Exam 1 ReviewJennifer PortilloÎncă nu există evaluări
- Tinea UnguiumDocument8 paginiTinea UnguiumwirdahajaÎncă nu există evaluări
- Respiratory System Functions and DisordersDocument7 paginiRespiratory System Functions and DisordersWeinston Tapayan BayonÎncă nu există evaluări
- Ikhlas Muhammad Jenie Physiology Department: Fkik UmyDocument43 paginiIkhlas Muhammad Jenie Physiology Department: Fkik UmyAnnisa FitrianiÎncă nu există evaluări
- The Respiratory System: Lower Airway Disorders and PneumoniaDocument247 paginiThe Respiratory System: Lower Airway Disorders and PneumoniaKatrina PonceÎncă nu există evaluări
- Ikhlas Muhammad Jenie Physiology Department: Fkik UmyDocument56 paginiIkhlas Muhammad Jenie Physiology Department: Fkik Umyade ayuningsih utamiÎncă nu există evaluări
- Respi NCM102Document126 paginiRespi NCM102Kristine BravoÎncă nu există evaluări
- COPD Case PresentationDocument50 paginiCOPD Case PresentationSarah Ann Jamilla FaciolanÎncă nu există evaluări
- Disorders of Oxygenation Spring 17Document94 paginiDisorders of Oxygenation Spring 17Cruz YrÎncă nu există evaluări
- COPDDocument6 paginiCOPDAubrey PerezÎncă nu există evaluări
- Astma Concept MapDocument1 paginăAstma Concept MapmikeÎncă nu există evaluări
- SS Visser, Pulmonology Internal Medicine UPDocument33 paginiSS Visser, Pulmonology Internal Medicine UPRonnie JaderÎncă nu există evaluări
- Manage Asthma in Children EffectivelyDocument50 paginiManage Asthma in Children EffectivelyG SÎncă nu există evaluări
- MRCP Paces Chest RedclifffDocument13 paginiMRCP Paces Chest RedclifffIsmail H AÎncă nu există evaluări
- COPDDocument49 paginiCOPDArmoured SpartanÎncă nu există evaluări
- Week 3 Obstructive DisorderDocument79 paginiWeek 3 Obstructive Disorderdelrosariojm87Încă nu există evaluări
- COPD GuideDocument44 paginiCOPD GuideNaresh JeengarÎncă nu există evaluări
- AsthmaDocument6 paginiAsthmaJay Hipulan QuiranteÎncă nu există evaluări
- Physiology of Nose & P.N.S.: Dr. Vishal SharmaDocument54 paginiPhysiology of Nose & P.N.S.: Dr. Vishal SharmaE=MC2Încă nu există evaluări
- Current Management of Asthma 2Document43 paginiCurrent Management of Asthma 2dan ekelemeÎncă nu există evaluări
- Nutrition and Respiratory Diseases PDFDocument53 paginiNutrition and Respiratory Diseases PDFliggiedy100% (1)
- Resume Skenario 5 - Tutorial HDocument46 paginiResume Skenario 5 - Tutorial HMuhammad FakhrizalÎncă nu există evaluări
- Lung conditions: Atelectasis, tuberculosis, abscess and pleural effusionDocument14 paginiLung conditions: Atelectasis, tuberculosis, abscess and pleural effusionSasha IfahmyÎncă nu există evaluări
- 06 Respiratory03 Patho02Document46 pagini06 Respiratory03 Patho02Divyajyoti DevaÎncă nu există evaluări
- ARDS (Dr. Edi Nurtjahja - SP.P)Document23 paginiARDS (Dr. Edi Nurtjahja - SP.P)Mirna Ayu Permata SariÎncă nu există evaluări
- Chronic Obstructive Pulmonary DiseaseDocument48 paginiChronic Obstructive Pulmonary DiseaseddallasÎncă nu există evaluări
- Chronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredDocument25 paginiChronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredOmar AbdillahiÎncă nu există evaluări
- 2nd Lecture Chest and LowerDocument18 pagini2nd Lecture Chest and LowerChucky VergaraÎncă nu există evaluări
- ARDSDocument43 paginiARDSJose PerdikaÎncă nu există evaluări
- NUR5703 Respiratory Advanced PathophysiologyDocument16 paginiNUR5703 Respiratory Advanced PathophysiologyLee MeyerÎncă nu există evaluări
- Anaesthesia For Patients With COPD: University College of Medical Sciences & GTB Hospital, DelhiDocument76 paginiAnaesthesia For Patients With COPD: University College of Medical Sciences & GTB Hospital, DelhiRINI100% (1)
- COPD Guide: Chronic Obstructive Pulmonary Disease OverviewDocument50 paginiCOPD Guide: Chronic Obstructive Pulmonary Disease OverviewNaresh JeengarÎncă nu există evaluări
- Defense Mechanism of Respiratory Tract: Winarti Bagian/SMF Patologi Anatomi FK UnudDocument35 paginiDefense Mechanism of Respiratory Tract: Winarti Bagian/SMF Patologi Anatomi FK Unuddr.Dewi ShintaherÎncă nu există evaluări
- PNEUMONIA: CAUSES, SYMPTOMS, AND TREATMENTDocument25 paginiPNEUMONIA: CAUSES, SYMPTOMS, AND TREATMENTDayu MandhaÎncă nu există evaluări
- Infeksi Saluran Napas BawahDocument54 paginiInfeksi Saluran Napas Bawahfahri somantriÎncă nu există evaluări
- Chronic Bronchitis, Emphysema, Bronciectasis - PPT.Document51 paginiChronic Bronchitis, Emphysema, Bronciectasis - PPT.Jumar ValdezÎncă nu există evaluări
- Chronic Obstructive Pulmonary DiseaseDocument45 paginiChronic Obstructive Pulmonary DiseaseAlexander Santiago ParelÎncă nu există evaluări
- Ards PDFDocument73 paginiArds PDFdr.Nugroho PrasetyoÎncă nu există evaluări
- Asthma and COPDDocument28 paginiAsthma and COPDShoaib PatelÎncă nu există evaluări
- Kardiorespirasi 5Document83 paginiKardiorespirasi 5Naufal MubarakÎncă nu există evaluări
- COPD and Lung CancerDocument42 paginiCOPD and Lung CancerENKELI VALDECANTOSÎncă nu există evaluări
- Neonatal Acute Respiratory Distress Syndrome (RDS) ManagementDocument30 paginiNeonatal Acute Respiratory Distress Syndrome (RDS) ManagementSanjay Kumar Sanju100% (1)
- Smoking: COPD - Chronic Obstructive Pulmonary DiseaseDocument2 paginiSmoking: COPD - Chronic Obstructive Pulmonary DiseaseRain MarquezÎncă nu există evaluări
- Farmakoterapi PPOK PDFDocument61 paginiFarmakoterapi PPOK PDFElizabeth SniderÎncă nu există evaluări
- ABC of Chronic Obstructive Pulmonary Disease Pathology, Pathogenesis, and PathophysiologyDocument3 paginiABC of Chronic Obstructive Pulmonary Disease Pathology, Pathogenesis, and PathophysiologyLorena SegoviaÎncă nu există evaluări
- Respiratory Disorders Pedia 1Document94 paginiRespiratory Disorders Pedia 1Jamaica CapunongÎncă nu există evaluări
- Burns - Airway Clearance, Risk For IneffectiveDocument2 paginiBurns - Airway Clearance, Risk For Ineffectivemakyofrancis20Încă nu există evaluări
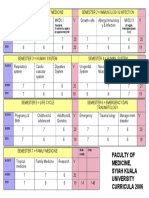
- Faculty of Medicine, Syiah Kuala University Curricula 2006Document1 paginăFaculty of Medicine, Syiah Kuala University Curricula 2006wirdahajaÎncă nu există evaluări
- Diagnosis Banding Berbak Merah Kulit dan Diagnosis DifferensialDocument7 paginiDiagnosis Banding Berbak Merah Kulit dan Diagnosis DifferensialHari PranotoÎncă nu există evaluări
- Acute Rheumatic FeverDocument39 paginiAcute Rheumatic FeverwirdahajaÎncă nu există evaluări
- DIG Trauma HeparDocument37 paginiDIG Trauma HeparwirdahajaÎncă nu există evaluări
- Atopic DermatitisDocument19 paginiAtopic DermatitiswirdahajaÎncă nu există evaluări
- Diagnosis Banding Berbak Merah Kulit dan Diagnosis DifferensialDocument7 paginiDiagnosis Banding Berbak Merah Kulit dan Diagnosis DifferensialHari PranotoÎncă nu există evaluări
- Metabolic EncephalopathyDocument26 paginiMetabolic Encephalopathywirdahaja100% (3)
- TOEFL TEST Dan Kunci JawabanDocument5 paginiTOEFL TEST Dan Kunci JawabanwirdahajaÎncă nu există evaluări
- IRIS Retina ExplanationsDocument19 paginiIRIS Retina ExplanationsBalraj GangadharÎncă nu există evaluări
- Microbiology - Scabies and PediculosisDocument32 paginiMicrobiology - Scabies and PediculosiswirdahajaÎncă nu există evaluări
- Fever and RashDocument14 paginiFever and RashwirdahajaÎncă nu există evaluări
- Metabolic EncephalopathyDocument26 paginiMetabolic Encephalopathywirdahaja100% (3)
- Anatomy of The Ear HearingDocument14 paginiAnatomy of The Ear HearingwirdahajaÎncă nu există evaluări
- Cole StasisDocument59 paginiCole StasiswirdahajaÎncă nu există evaluări
- ABSES HATI-SytDocument29 paginiABSES HATI-SytwirdahajaÎncă nu există evaluări
- Managing Abdominal Pain: A Guide for Diagnosis and TreatmentDocument38 paginiManaging Abdominal Pain: A Guide for Diagnosis and TreatmentSusi Muharni RismaÎncă nu există evaluări
- Follow Up: No Tanggal Subjektif Objektif Assessment Planning TerapiDocument4 paginiFollow Up: No Tanggal Subjektif Objektif Assessment Planning TerapiwirdahajaÎncă nu există evaluări
- Secondary SyphilisDocument2 paginiSecondary SyphilisRoberto López MataÎncă nu există evaluări
- Peptic Ulcer and GERD: Chiao-Hsiung ChuangDocument58 paginiPeptic Ulcer and GERD: Chiao-Hsiung ChuangMK CameraÎncă nu există evaluări
- Lisa Black InterviewDocument4 paginiLisa Black InterviewPrezioIAHCSMMÎncă nu există evaluări
- Medication Guidelines Vol 1 Antimicrobial Prescribing v1.1 1Document77 paginiMedication Guidelines Vol 1 Antimicrobial Prescribing v1.1 1doodrillÎncă nu există evaluări
- Chapter 21 HomeworkDocument12 paginiChapter 21 HomeworkKvn4N6Încă nu există evaluări
- Vere Chip TMDocument12 paginiVere Chip TMRubi RubiandaniÎncă nu există evaluări
- ISCAID Urinary GuidelinesDocument9 paginiISCAID Urinary Guidelinesartzain1991Încă nu există evaluări
- GGT Test GGTP Gamma-GT GTP Gamma-Glutamyl Transferase Gamma-Glutamyl Transpeptidase - Lab Tests OnlineDocument4 paginiGGT Test GGTP Gamma-GT GTP Gamma-Glutamyl Transferase Gamma-Glutamyl Transpeptidase - Lab Tests OnlinechichavlajaÎncă nu există evaluări
- Osteolytic LesionsDocument20 paginiOsteolytic LesionsVineel BezawadaÎncă nu există evaluări
- Bacteriophage & Lytic Cycle RelationshipDocument5 paginiBacteriophage & Lytic Cycle RelationshipOmar Mohsen SarhanÎncă nu există evaluări
- Doxycyclin Alkaloid 100mg Capsules - ZIDocument12 paginiDoxycyclin Alkaloid 100mg Capsules - ZIMaja TrajanovikjÎncă nu există evaluări
- Acute Hematogenous Osteomyelitis in ChildrenDocument63 paginiAcute Hematogenous Osteomyelitis in ChildrenCati Moraru100% (1)
- What Is HIV, It's Symptoms, Causes and Treatment - MeddcoDocument9 paginiWhat Is HIV, It's Symptoms, Causes and Treatment - MeddcoMeddco HealthcareÎncă nu există evaluări
- Nosocomial Infections For BSN 2021Document48 paginiNosocomial Infections For BSN 2021Muhammad SheerazÎncă nu există evaluări
- Infective EndocarditisDocument29 paginiInfective EndocarditistmtatroÎncă nu există evaluări
- 2007 Scope Reprocessing Competency PackageDocument88 pagini2007 Scope Reprocessing Competency PackageAnonymous YIAOYoÎncă nu există evaluări
- THE HELMINTHS: KEY PARASITIC WORMSDocument9 paginiTHE HELMINTHS: KEY PARASITIC WORMSMomo ShinÎncă nu există evaluări
- Basics On Test Selection For Parasites in The CatDocument4 paginiBasics On Test Selection For Parasites in The CatChantelle NeufeldÎncă nu există evaluări
- Lumpy Skin Disease FinalDocument5 paginiLumpy Skin Disease FinalrohishaakÎncă nu există evaluări
- Biological Safety in LaboratorieDocument94 paginiBiological Safety in Laboratoriem.abdullahÎncă nu există evaluări
- 4.daftar PustakaDocument8 pagini4.daftar PustakaTsania MahiraÎncă nu există evaluări
- Malaria Is A Mosquito-Borne Infectious Disease of Humans and OtherDocument3 paginiMalaria Is A Mosquito-Borne Infectious Disease of Humans and Otherkiran PoudelÎncă nu există evaluări
- Enzyme Catalase LabDocument4 paginiEnzyme Catalase Labluckyduck2869Încă nu există evaluări
- COVID-19 THREATENS YOUNG PEOPLE TOODocument5 paginiCOVID-19 THREATENS YOUNG PEOPLE TOONgô Minh Khuê- Lớp 9/4Încă nu există evaluări