S-ar putea să vă placă și
- The Illustrated Book of Medicine: The Making of MeDe la EverandThe Illustrated Book of Medicine: The Making of MeÎncă nu există evaluări
- Lecture 1physiology of PregnancyDocument58 paginiLecture 1physiology of PregnancyОлександра ЗагородняÎncă nu există evaluări
- Lecture 1A Genetics Conception Fall 2015 Student'sDocument49 paginiLecture 1A Genetics Conception Fall 2015 Student'sDurgaÎncă nu există evaluări
- IVF Unveiled: A Comprehensive Guide to Fertility TreatmentsDe la EverandIVF Unveiled: A Comprehensive Guide to Fertility TreatmentsÎncă nu există evaluări
- Conception Fetal Development & Genetics: Mary L. Dunlap MSN, Fall 2015Document49 paginiConception Fetal Development & Genetics: Mary L. Dunlap MSN, Fall 2015DurgaÎncă nu există evaluări
- Extragenital Pathology and Pregnancy Perinatal MedicineDocument178 paginiExtragenital Pathology and Pregnancy Perinatal MedicineSthefanie Rocha GouveiaÎncă nu există evaluări
- Fertilization and Fetal Development Abd CirculiationDocument54 paginiFertilization and Fetal Development Abd CirculiationMohnnad Hmood AlgaraybhÎncă nu există evaluări
- 1. 1st&2nd weekDocument38 pagini1. 1st&2nd weekJeniÎncă nu există evaluări
- Normal PregnancyDocument86 paginiNormal PregnancygayleesinfuegoÎncă nu există evaluări
- 1st 02nd WeekDocument44 pagini1st 02nd WeekMajd HusseinÎncă nu există evaluări
- Competency 1-The Family Before Birth: 1. Explain The Structure and Function of The Female Reproductive SystemDocument4 paginiCompetency 1-The Family Before Birth: 1. Explain The Structure and Function of The Female Reproductive SystemEnorl FerdinandÎncă nu există evaluări
- Day 2 Review Pregnancy Fetal Development and Labor and DeliveryDocument84 paginiDay 2 Review Pregnancy Fetal Development and Labor and DeliveryInah SaritaÎncă nu există evaluări
- Female Reproductive BiologyDocument57 paginiFemale Reproductive BiologyYunes AryoÎncă nu există evaluări
- Multiple PregnancyDocument15 paginiMultiple PregnancyM.S.H TubeÎncă nu există evaluări
- Lect12 - Amniotic Fluid ModifiedDocument22 paginiLect12 - Amniotic Fluid Modifiedyelisetti DakshayaniÎncă nu există evaluări
- Sexual Response Fertiliztion ImplantationembryoDocument38 paginiSexual Response Fertiliztion ImplantationembryoHana-Lou TaquiquiÎncă nu există evaluări
- Understanding Pregnancy and ParenthoodDocument36 paginiUnderstanding Pregnancy and ParenthoodAjay Kumar AtluriÎncă nu există evaluări
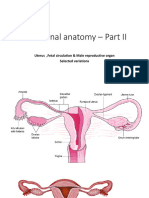
- Functional Anatomy - Part II: Uterus, Fetal Circulation & Male Reproductive Organ Selected VariationsDocument69 paginiFunctional Anatomy - Part II: Uterus, Fetal Circulation & Male Reproductive Organ Selected Variationshfkxbbbty2Încă nu există evaluări
- Placenta FunctionsDocument46 paginiPlacenta Functionsvenkata sryanamala50% (2)
- Clinical Activities: A. Pre - ConsultationDocument13 paginiClinical Activities: A. Pre - ConsultationerykafadsÎncă nu există evaluări
- Pregnancy - Human ReproductionDocument36 paginiPregnancy - Human ReproductionDICKSONÎncă nu există evaluări
- Rhesus ObgynDocument44 paginiRhesus Obgynpatboothe1880Încă nu există evaluări
- Genetic, Conception, and Fetal DevelopmentDocument54 paginiGenetic, Conception, and Fetal DevelopmentBiraito TakanaÎncă nu există evaluări
- Pregnancy MarkersDocument34 paginiPregnancy MarkersAbeer AhmedÎncă nu există evaluări
- Placenta & Fetal CirculationDocument32 paginiPlacenta & Fetal CirculationFarxan Da Napolian BwoyÎncă nu există evaluări
- Anatomi dan Fisiologi Kehamilan dan PersalinanDocument60 paginiAnatomi dan Fisiologi Kehamilan dan PersalinanBimantoro SaputroÎncă nu există evaluări
- Assisted Reproductive TechnologyDocument14 paginiAssisted Reproductive Technologyarchana jainÎncă nu există evaluări
- Prenatal DevelopmentDocument33 paginiPrenatal DevelopmentKarl MesinaÎncă nu există evaluări
- Fertilitas Dan Infertilitas: BY Tettisolehati, S.KP., M.KepDocument32 paginiFertilitas Dan Infertilitas: BY Tettisolehati, S.KP., M.KepAny AndrianiÎncă nu există evaluări
- Diagnostic ApprDocument33 paginiDiagnostic ApprNicole ArandingÎncă nu există evaluări
- Vaginal Bleeding During PregnancyDocument67 paginiVaginal Bleeding During PregnancyLunaLureÎncă nu există evaluări
- Hydatidiform-Mole-FINAL-NA-TALAGAAA (AutoRecovered)Document25 paginiHydatidiform-Mole-FINAL-NA-TALAGAAA (AutoRecovered)Lezel LaracasÎncă nu există evaluări
- Fertility and Infertility Factors in Men and WomenDocument32 paginiFertility and Infertility Factors in Men and WomenWindy Shintia FandinyÎncă nu există evaluări
- REVIEWERDocument7 paginiREVIEWERKhaskie Geneva DumaguinÎncă nu există evaluări
- Maternity 1Document7 paginiMaternity 1janet rooseveltÎncă nu există evaluări
- ANATOMI - Chapter25ReproFemaleMariebDocument30 paginiANATOMI - Chapter25ReproFemaleMariebAdhi TjahyadiÎncă nu există evaluări
- How the Placenta Supports Fetal GrowthDocument4 paginiHow the Placenta Supports Fetal GrowthJoanne LauÎncă nu există evaluări
- The Growing FetusDocument62 paginiThe Growing Fetuscoosa liquorsÎncă nu există evaluări
- Human Reproduction and Development NotesDocument7 paginiHuman Reproduction and Development Notesennes9141Încă nu există evaluări
- Reproduction and HeredityDocument10 paginiReproduction and HeredityMonkey LoverÎncă nu există evaluări
- 4 Family Having Difficulty Conceiving A ChildDocument10 pagini4 Family Having Difficulty Conceiving A ChildDrex CuritanaÎncă nu există evaluări
- CXC BIOLOGY LECTURE SERIES COVERS KEY TOPICSDocument58 paginiCXC BIOLOGY LECTURE SERIES COVERS KEY TOPICSShantay BurtonÎncă nu există evaluări
- Assisted Reproductive Technologies (ART) : Doaa HegabDocument23 paginiAssisted Reproductive Technologies (ART) : Doaa HegabLinguum100% (1)
- Fetal and Placental Physiology:: The PlacentaDocument14 paginiFetal and Placental Physiology:: The PlacentaTri GunawanÎncă nu există evaluări
- Sex Hormones: Female Reproduction Male ReproductionDocument113 paginiSex Hormones: Female Reproduction Male ReproductionM HUSSAINÎncă nu există evaluări
- Lesson 2 NCM 107aDocument5 paginiLesson 2 NCM 107aInsatiable CleeÎncă nu există evaluări
- 5 Normal PeurpuriumDocument48 pagini5 Normal Peurpuriumdemeke andebetÎncă nu există evaluări
- Ectopic PregnancyDocument36 paginiEctopic PregnancyLorenz BreezÎncă nu există evaluări
- Fertilization and Implantation Copy To StudentsDocument40 paginiFertilization and Implantation Copy To StudentsRiya SinghÎncă nu există evaluări
- Semi Finals CHAPTER IVDocument5 paginiSemi Finals CHAPTER IVjacobprince0016Încă nu există evaluări
- Pregnancy N Lactation: Dr. Javaria LatifDocument41 paginiPregnancy N Lactation: Dr. Javaria LatifSyeda Naveen BatoolÎncă nu există evaluări
- Multiple PXDocument46 paginiMultiple PXBetelhem EjiguÎncă nu există evaluări
- INFERTILITYDocument67 paginiINFERTILITYIsaacÎncă nu există evaluări
- Treatment of InfertilityDocument22 paginiTreatment of InfertilityAlina ShahÎncă nu există evaluări
- Mother and Child Health: Theories of Procreation and Human ReproductionDocument390 paginiMother and Child Health: Theories of Procreation and Human ReproductionJeonghwa Park100% (1)
- Science Class Explains Reproductive Health IssuesDocument72 paginiScience Class Explains Reproductive Health IssuesLance Andre V. RosalÎncă nu există evaluări
- Fertilization, Pregnancy and Lactation: Dedi ArdinataDocument26 paginiFertilization, Pregnancy and Lactation: Dedi ArdinataHalseyÎncă nu există evaluări
- Embryo Transfer TechnologyDocument49 paginiEmbryo Transfer TechnologyshubhÎncă nu există evaluări
- Introduction To Embryology.Document24 paginiIntroduction To Embryology.Mercy AdeolaÎncă nu există evaluări
- Basics of Female Reproduction (39Document9 paginiBasics of Female Reproduction (39Jestoni Dulva ManiagoÎncă nu există evaluări
- PRISMA 2009 Checklist: An AnalysisDocument2 paginiPRISMA 2009 Checklist: An AnalysisFiŗåš ÀßßâşÎncă nu există evaluări
- Maternal Mortality SaudiDocument5 paginiMaternal Mortality SaudiJestoni Dulva ManiagoÎncă nu există evaluări
- Unit 4-5 Searching The Evidence and Its ApplicationDocument12 paginiUnit 4-5 Searching The Evidence and Its ApplicationJestoni Dulva ManiagoÎncă nu există evaluări
- Cultural DiversityDocument35 paginiCultural DiversityJestoni Dulva ManiagoÎncă nu există evaluări
- Learning Styles Kolb QuestionnaireDocument6 paginiLearning Styles Kolb QuestionnaireAkshay BellubbiÎncă nu există evaluări
- Nursing Care of The NewbornDocument34 paginiNursing Care of The NewbornJestoni Dulva ManiagoÎncă nu există evaluări
- History of NursingDocument38 paginiHistory of NursingJestoni Dulva ManiagoÎncă nu există evaluări
- Nursing TBTB1Document104 paginiNursing TBTB1ptkduong100% (1)
- OLDS Week2 QwizdomDocument142 paginiOLDS Week2 QwizdomJestoni Dulva ManiagoÎncă nu există evaluări
- Kolblearningsurvey PDFDocument2 paginiKolblearningsurvey PDFJestoni Dulva ManiagoÎncă nu există evaluări
- Kolb LSI PDFDocument5 paginiKolb LSI PDFJestoni Dulva ManiagoÎncă nu există evaluări
- GastroDocument23 paginiGastroJestoni Dulva ManiagoÎncă nu există evaluări
- 40ch Chest ExamDocument19 pagini40ch Chest ExamJestoni Dulva ManiagoÎncă nu există evaluări
- 40ch Chest ExamDocument19 pagini40ch Chest ExamJestoni Dulva ManiagoÎncă nu există evaluări
- Abbreviations Commonly Used in Obstetrics and Gynecology Physical ExaminationDocument2 paginiAbbreviations Commonly Used in Obstetrics and Gynecology Physical ExaminationwenwenwencheatÎncă nu există evaluări
- Ch04, 05 & 08Document53 paginiCh04, 05 & 08Jestoni Dulva ManiagoÎncă nu există evaluări
- Lecture 1 NotesDocument14 paginiLecture 1 NotesJestoni Dulva ManiagoÎncă nu există evaluări
- Bioethical PrinciplesDocument4 paginiBioethical PrinciplesJestoni Dulva ManiagoÎncă nu există evaluări
- Research B (Research Proposal Matrix)Document9 paginiResearch B (Research Proposal Matrix)Jestoni Dulva ManiagoÎncă nu există evaluări
- Man 204 PrimerDocument38 paginiMan 204 PrimerJestoni Dulva ManiagoÎncă nu există evaluări
- ORID FormatDocument1 paginăORID FormatJestoni Dulva ManiagoÎncă nu există evaluări
- LOGIC - Lecture 01Document3 paginiLOGIC - Lecture 01Jestoni Dulva ManiagoÎncă nu există evaluări
- 3-Way ANOVA Factors Learning ErrorsDocument21 pagini3-Way ANOVA Factors Learning ErrorsJestoni Dulva ManiagoÎncă nu există evaluări
- Outline On Human DevelopementDocument15 paginiOutline On Human Developementkell73kÎncă nu există evaluări
- LOGIC - Lecture 02Document1 paginăLOGIC - Lecture 02Jestoni Dulva ManiagoÎncă nu există evaluări
- LOGIC - Lecture 01Document3 paginiLOGIC - Lecture 01Jestoni Dulva ManiagoÎncă nu există evaluări
- Report (Curriculum Development)Document5 paginiReport (Curriculum Development)Jestoni Dulva ManiagoÎncă nu există evaluări
- Critical Thinking Practice ExercisesDocument2 paginiCritical Thinking Practice ExercisesJestoni Dulva ManiagoÎncă nu există evaluări