S-ar putea să vă placă și
- Curriculum Vitae: Personal DetailsDocument3 paginiCurriculum Vitae: Personal DetailsBibek RajÎncă nu există evaluări
- When Is Oral Biopsy Not Needed?Document6 paginiWhen Is Oral Biopsy Not Needed?Bibek RajÎncă nu există evaluări
- For Mucocele Lesions - Careful Excisional BiopsyDocument11 paginiFor Mucocele Lesions - Careful Excisional BiopsyBibek RajÎncă nu există evaluări
- QDWPlicDocument2 paginiQDWPlicBibek RajÎncă nu există evaluări
- 3 UhnjkcDocument8 pagini3 UhnjkcBibek RajÎncă nu există evaluări
- JdsmcxnksDocument32 paginiJdsmcxnksBibek RajÎncă nu există evaluări
- Inflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryDocument73 paginiInflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryBibek RajÎncă nu există evaluări
- Background Methods: Review' (OHAR) Guidance in BriefDocument1 paginăBackground Methods: Review' (OHAR) Guidance in BriefBibek RajÎncă nu există evaluări
- Biopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Document5 paginiBiopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Bibek RajÎncă nu există evaluări
- Practical Skill Station Basic Life Support Key Teaching ObjectivesDocument3 paginiPractical Skill Station Basic Life Support Key Teaching ObjectivesBibek RajÎncă nu există evaluări
- Trapezoidal Flap. A Diagrammatic IllustrationDocument6 paginiTrapezoidal Flap. A Diagrammatic IllustrationBibek RajÎncă nu există evaluări
- DhdifogkDocument4 paginiDhdifogkBibek RajÎncă nu există evaluări
- JDJDJDJDocument23 paginiJDJDJDJBibek RajÎncă nu există evaluări
- DrtfygbyuijDocument29 paginiDrtfygbyuijBibek RajÎncă nu există evaluări
- Vitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsDocument6 paginiVitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsBibek RajÎncă nu există evaluări
- Background Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieDocument1 paginăBackground Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieBibek RajÎncă nu există evaluări
- YuybnunhhuhbDocument2 paginiYuybnunhhuhbBibek RajÎncă nu există evaluări
- FfghhthjgvyujhDocument1 paginăFfghhthjgvyujhBibek RajÎncă nu există evaluări
- Ultrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationDocument2 paginiUltrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationBibek RajÎncă nu există evaluări
- YudsbhcjDocument1 paginăYudsbhcjBibek RajÎncă nu există evaluări
- Rapid: Reducing Antibiotic Prescribing in DentistryDocument5 paginiRapid: Reducing Antibiotic Prescribing in DentistryBibek RajÎncă nu există evaluări
- TG 6 YhunjDocument48 paginiTG 6 YhunjBibek RajÎncă nu există evaluări
- Warfarin and Your Dental Treatment: Information For PatientsDocument5 paginiWarfarin and Your Dental Treatment: Information For PatientsBibek RajÎncă nu există evaluări
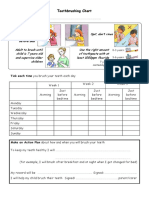
- Toothbrushing Chart PDFDocument1 paginăToothbrushing Chart PDFBibek RajÎncă nu există evaluări
- Dental Anxiety Form 4 PDFDocument2 paginiDental Anxiety Form 4 PDFBibek RajÎncă nu există evaluări
- VfyggdbDocument33 paginiVfyggdbBibek RajÎncă nu există evaluări
- Toothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayDocument1 paginăToothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayBibek RajÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Learning Through PlayDocument2 paginiLearning Through PlayThe American Occupational Therapy Association100% (1)
- OPD Claim Form 2020Document1 paginăOPD Claim Form 2020RafayÎncă nu există evaluări
- Therapeutic Gases 9.3.17 and CoughDocument29 paginiTherapeutic Gases 9.3.17 and CoughThor O100% (1)
- Body Image ScaleDocument9 paginiBody Image ScaleMicah MatibagÎncă nu există evaluări
- Critical Care Nursing A Holistic Approach 11th Edition Morton Fontaine Test Bank PDFDocument335 paginiCritical Care Nursing A Holistic Approach 11th Edition Morton Fontaine Test Bank PDFSami Atawi100% (1)
- National Antibiotic Guideline 2014 Full Versionjun2015 - 1 PDFDocument247 paginiNational Antibiotic Guideline 2014 Full Versionjun2015 - 1 PDFfghjÎncă nu există evaluări
- Venipunture ProcedureDocument4 paginiVenipunture ProcedureAnusha VergheseÎncă nu există evaluări
- SOP TEC 15 Calculating Drug Doses v1.1Document2 paginiSOP TEC 15 Calculating Drug Doses v1.1rajenderizeÎncă nu există evaluări
- Paracetamol PKPD Drugs PDFDocument10 paginiParacetamol PKPD Drugs PDFFahmi M FaturahmanÎncă nu există evaluări
- Learning Plan Tle 9 Nail Care NewDocument9 paginiLearning Plan Tle 9 Nail Care NewJoselito CepadaÎncă nu există evaluări
- Assessment Tool 2Document14 paginiAssessment Tool 2karenkaren09Încă nu există evaluări
- Aromatherapy & DepressionDocument3 paginiAromatherapy & DepressionTheMothershipÎncă nu există evaluări
- Current Issues & Trends in Older: Persons Chronic CareDocument12 paginiCurrent Issues & Trends in Older: Persons Chronic CareKeepItSecretÎncă nu există evaluări
- Cyclic Progesterone Therapy Patient HandoutDocument1 paginăCyclic Progesterone Therapy Patient HandoutMuhammadRizalNÎncă nu există evaluări
- S1 Hippocratic Oath Seminar and Reading NotesDocument7 paginiS1 Hippocratic Oath Seminar and Reading NotesTaraSubba1995Încă nu există evaluări
- Medicinal Chemistry: The Molecular Basis of Drug Discovery: Khan AcademyDocument17 paginiMedicinal Chemistry: The Molecular Basis of Drug Discovery: Khan AcademyRinta MoonÎncă nu există evaluări
- Meloxicam 7.5 MG Daily and Naproxen 750Document7 paginiMeloxicam 7.5 MG Daily and Naproxen 750kwadwobrosÎncă nu există evaluări
- Insulin IndexDocument13 paginiInsulin IndexbookbookpdfÎncă nu există evaluări
- May 20151Document17 paginiMay 20151Hany Rasheed Mohamed50% (2)
- Finalpaper SchnakeDocument6 paginiFinalpaper Schnakeapi-315989347Încă nu există evaluări
- Case Study of Most Common Communicable DiseasesDocument13 paginiCase Study of Most Common Communicable DiseasesnesjynÎncă nu există evaluări
- (Hema Manucript) Myelophthisic Anemia FINALCMPDocument6 pagini(Hema Manucript) Myelophthisic Anemia FINALCMPJohney Doe100% (1)
- Ayurvedic Treatment of Malaria in Hindi Ilaj Ke 10 Aasan UpayDocument3 paginiAyurvedic Treatment of Malaria in Hindi Ilaj Ke 10 Aasan UpayGovindÎncă nu există evaluări
- Schizoaffective DisorderDocument8 paginiSchizoaffective DisorderKaren Gail ComiaÎncă nu există evaluări
- 5 Day Bodybuilding Workout ScheduleDocument4 pagini5 Day Bodybuilding Workout ScheduleNazri Yusoff100% (1)
- Physical Therapy For Neurological Disorders (2) 2Document11 paginiPhysical Therapy For Neurological Disorders (2) 2Muskan AhujaÎncă nu există evaluări
- Clinical Efficacy of Mechanical Traction As Physical Therapy For Lumbar Disc Herniation - Meta AnalysisDocument8 paginiClinical Efficacy of Mechanical Traction As Physical Therapy For Lumbar Disc Herniation - Meta AnalysissamÎncă nu există evaluări
- NCP AssigmentDocument18 paginiNCP AssigmentMuhammad Na'imÎncă nu există evaluări
- Anaesthesia TMJ Pain Orthognathic Pathology ReconstructionDocument220 paginiAnaesthesia TMJ Pain Orthognathic Pathology ReconstructionMohammed Qasim Al-Watary67% (3)
- NCP-DP NCM112LecDocument4 paginiNCP-DP NCM112LecShane CabucosÎncă nu există evaluări