S-ar putea să vă placă și
- Alert Medical Series: Emergency Medicine Alert IIIDe la EverandAlert Medical Series: Emergency Medicine Alert IIIÎncă nu există evaluări
- OrganophosphateDocument21 paginiOrganophosphatehendra_darmawan_4Încă nu există evaluări
- Organophosphate PoisoningDocument31 paginiOrganophosphate Poisoningjosecarlo_masangkay100% (1)
- Clinical Pharmacology, Toxicology and Poisoning: 1. Drug Metabolism and InteractionsDocument26 paginiClinical Pharmacology, Toxicology and Poisoning: 1. Drug Metabolism and InteractionsNadia Ancharuz100% (1)
- Pharmacology of Adrenergic AgonistsDocument9 paginiPharmacology of Adrenergic Agonistsfiena92Încă nu există evaluări
- Comprehensive Study of Beta BlockersDocument40 paginiComprehensive Study of Beta Blockersapi-369859880% (5)
- HX TakingDocument37 paginiHX TakingAya SalahÎncă nu există evaluări
- Organophosphate Poisoning ManagementDocument31 paginiOrganophosphate Poisoning ManagementLIDIYA MOL P VÎncă nu există evaluări
- Krok 05-18Document312 paginiKrok 05-18Purwa Rane100% (1)
- Anti-Fungal Drugs - KatzungDocument2 paginiAnti-Fungal Drugs - Katzungsarguss14100% (2)
- MCEM Toxicology MCQDocument110 paginiMCEM Toxicology MCQAnkita Sinha100% (4)
- BURNS INITIAL EVALUATION GUIDEDocument80 paginiBURNS INITIAL EVALUATION GUIDEmarÎncă nu există evaluări
- Heart Failure Pathophysiology and Treatment OverviewDocument8 paginiHeart Failure Pathophysiology and Treatment Overviewcarlo_nonÎncă nu există evaluări
- Pulmonary FibrosisDocument39 paginiPulmonary FibrosisMarcoÎncă nu există evaluări
- CNS Pathology SummaryDocument38 paginiCNS Pathology Summaryimeds100% (2)
- Arrhythmia: Presenter-Dr Praveen Kumar Moderator - DR Sandhya ChauhanDocument71 paginiArrhythmia: Presenter-Dr Praveen Kumar Moderator - DR Sandhya ChauhanDr Praveen100% (1)
- Pharmacology of EthanolDocument5 paginiPharmacology of EthanolJoshua RemonÎncă nu există evaluări
- Chapter 13 Drugs Used in Heart FailureDocument7 paginiChapter 13 Drugs Used in Heart FailureChristine Annmarie TapawanÎncă nu există evaluări
- Anemia in ChildrenDocument9 paginiAnemia in ChildrenVillegas Sepúlveda AbrahamÎncă nu există evaluări
- Aminogycoside AntibioticsDocument31 paginiAminogycoside AntibioticsNurul Febrina100% (2)
- Y7PH0566, Yedla Pradeep Kumar, 4 B.Pharmacy, Cips, Lam, GunturDocument33 paginiY7PH0566, Yedla Pradeep Kumar, 4 B.Pharmacy, Cips, Lam, Gunturప్రదీప్ కుమార్100% (4)
- Pulmonary Patho PDFDocument623 paginiPulmonary Patho PDFNabeel Shahzad100% (1)
- Cardiac Emergencies Cne DelhiDocument109 paginiCardiac Emergencies Cne DelhiManisha Thakur100% (1)
- DiureticsDocument4 paginiDiureticsNazmul Islam AbirÎncă nu există evaluări
- Opportunistic Infections in HIVDocument50 paginiOpportunistic Infections in HIVamandaÎncă nu există evaluări
- Common Emergency DrugsDocument58 paginiCommon Emergency Drugshatem alsrour84% (19)
- Acid-Base Disorders NotesDocument10 paginiAcid-Base Disorders NotesLovely100% (1)
- Pulmonary Tuberculosis PharmacologyDocument48 paginiPulmonary Tuberculosis PharmacologyMarc Imhotep Cray, M.D.Încă nu există evaluări
- Anti Hypertensive Drugs - ACE InhibitorDocument16 paginiAnti Hypertensive Drugs - ACE InhibitorApurba Sarker Apu100% (1)
- Kidney TransplantationDocument14 paginiKidney TransplantationSujith KuttanÎncă nu există evaluări
- ER ToxicologyDocument17 paginiER ToxicologyasclswisconsinÎncă nu există evaluări
- Parapneumonic Pleural Effusions and Empyema Thoracis: Causes, Symptoms and TreatmentDocument4 paginiParapneumonic Pleural Effusions and Empyema Thoracis: Causes, Symptoms and TreatmentLorentina Den PanjaitanÎncă nu există evaluări
- Ischemic Heart DiseaseDocument8 paginiIschemic Heart DiseaseNina Natalia Bautista100% (1)
- Steroidal Anti - Inflammatory Drugs: NsaidsDocument96 paginiSteroidal Anti - Inflammatory Drugs: NsaidsDR AbidÎncă nu există evaluări
- Basic Pharmacology of DiureticsDocument46 paginiBasic Pharmacology of DiureticsMarc Imhotep Cray, M.D.100% (3)
- MRCP Guide Part 2Document351 paginiMRCP Guide Part 2Kuben Govender100% (2)
- Dr. Nilukshi Perera Consultant HaematologistDocument128 paginiDr. Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteÎncă nu există evaluări
- BMJ d2651 PDFDocument11 paginiBMJ d2651 PDFKarin KurniatiÎncă nu există evaluări
- Venous congestion in the liverDocument135 paginiVenous congestion in the liverJustin JannatiÎncă nu există evaluări
- Antiarrhythmic Drug Mechanisms and ClassificationDocument3 paginiAntiarrhythmic Drug Mechanisms and ClassificationPatrick Tan100% (1)
- Asthma: A Guide to the Heterogeneous DiseaseDocument18 paginiAsthma: A Guide to the Heterogeneous DiseaseSam HuntÎncă nu există evaluări
- Drugs Used in Heart Failure: Pharmacology (2) PHAR 342Document19 paginiDrugs Used in Heart Failure: Pharmacology (2) PHAR 342Dana HamarshehÎncă nu există evaluări
- Anticancer DrugsDocument26 paginiAnticancer DrugsNeha Chugh100% (1)
- Cerebrovascular Accident: TypesDocument10 paginiCerebrovascular Accident: TypesJulia SalvioÎncă nu există evaluări
- Adrenergic Agonists 2020 PDFDocument65 paginiAdrenergic Agonists 2020 PDFAlaa NaserÎncă nu există evaluări
- Arrhythmia Pharmacology MindmapDocument1 paginăArrhythmia Pharmacology MindmapTesnikolaÎncă nu există evaluări
- Drugs For Diabetes MellitusDocument3 paginiDrugs For Diabetes MellitusGerardLum100% (1)
- Multiple Myeloma: LT Col Vivek AggarwalDocument42 paginiMultiple Myeloma: LT Col Vivek AggarwalShravan Rakaraddi100% (2)
- PoisoningDocument103 paginiPoisoningC Hendra Wijaya100% (2)
- Community-Acquired Pneumonia Diagnosis and TreatmentDocument5 paginiCommunity-Acquired Pneumonia Diagnosis and TreatmentJerrica Charlene GalopeÎncă nu există evaluări
- FRCEM SAQ Intermediate Dec 2016 PDFDocument6 paginiFRCEM SAQ Intermediate Dec 2016 PDFsacabonaÎncă nu există evaluări
- Pericarditis 65 SlidesDocument65 paginiPericarditis 65 SlidesAtifBhoreÎncă nu există evaluări
- Beta BlockerDocument8 paginiBeta BlockerZiedTriki100% (1)
- HypertensionDocument15 paginiHypertensionHaidee Javier100% (3)
- CardiomyopathyDocument17 paginiCardiomyopathysarguss1450% (2)
- Central Nervous System Pharmacology: Elly Nurus SakinahDocument64 paginiCentral Nervous System Pharmacology: Elly Nurus Sakinahkareem92Încă nu există evaluări
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Organophospha Te (Op) Poisining: Presented byDocument44 paginiOrganophospha Te (Op) Poisining: Presented byShantanu Kr VatsyayanÎncă nu există evaluări
- Organophospha Te (Op) Poisining: Presented byDocument44 paginiOrganophospha Te (Op) Poisining: Presented byShantanu Kr VatsyayanÎncă nu există evaluări
- Chronic Renal Failure Long CaseDocument2 paginiChronic Renal Failure Long CaseUsman Ali AkbarÎncă nu există evaluări
- Chronic Renal Failure: Concise Long Case ApproachDocument3 paginiChronic Renal Failure: Concise Long Case ApproachUsman Ali AkbarÎncă nu există evaluări
- CRF Wtih Fluid Overload MX PathwayDocument1 paginăCRF Wtih Fluid Overload MX PathwayUsman Ali AkbarÎncă nu există evaluări
- Renal TransplantDocument2 paginiRenal TransplantUsman Ali AkbarÎncă nu există evaluări
- Obstructive Airway Diseases ExplainedDocument53 paginiObstructive Airway Diseases ExplainedUsman Ali AkbarÎncă nu există evaluări
- Polycystic Kidneys: Adult PKD: ComplicationsDocument1 paginăPolycystic Kidneys: Adult PKD: ComplicationsUsman Ali AkbarÎncă nu există evaluări
- Urinary Tract Infection & PyelonephritisDocument3 paginiUrinary Tract Infection & PyelonephritisUsman Ali AkbarÎncă nu există evaluări
- Renal Tubular Acidosis SummaryDocument1 paginăRenal Tubular Acidosis SummaryUsman Ali AkbarÎncă nu există evaluări
- Nephrotic SyndromeDocument2 paginiNephrotic SyndromeUsman Ali AkbarÎncă nu există evaluări
- Renal Tubular Acidosis Summary - AdjDocument1 paginăRenal Tubular Acidosis Summary - AdjUsman Ali AkbarÎncă nu există evaluări
- CRF Wtih Fluid Overload MX Pathway - AdjDocument1 paginăCRF Wtih Fluid Overload MX Pathway - AdjUsman Ali AkbarÎncă nu există evaluări
- Dialysis Treatment Options: Peritoneal Dialysis vs HemodialysisDocument2 paginiDialysis Treatment Options: Peritoneal Dialysis vs HemodialysisUsman Ali AkbarÎncă nu există evaluări
- Anaemia in PregnancyDocument13 paginiAnaemia in PregnancyUsman Ali AkbarÎncă nu există evaluări
- King Khalid University Hospital Department of Obstetrics & Gyncology Course 481Document40 paginiKing Khalid University Hospital Department of Obstetrics & Gyncology Course 481Usman Ali AkbarÎncă nu există evaluări
- GI Bleeding Team Work - 2nd EditionDocument9 paginiGI Bleeding Team Work - 2nd EditionUsman Ali AkbarÎncă nu există evaluări
- GRAM NEGATIVE RODS (5) Fastidious Organisms From Animal Sources (A)Document1 paginăGRAM NEGATIVE RODS (5) Fastidious Organisms From Animal Sources (A)Usman Ali AkbarÎncă nu există evaluări
- GI Bleeding Team Work - 2nd EditionDocument9 paginiGI Bleeding Team Work - 2nd EditionUsman Ali AkbarÎncă nu există evaluări
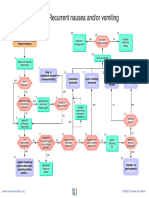
- Recurrent Nausea Andor VomitingDocument8 paginiRecurrent Nausea Andor VomitingUsman Ali AkbarÎncă nu există evaluări
- Subject: Permission For Badminton Court NID, Multan: TH THDocument1 paginăSubject: Permission For Badminton Court NID, Multan: TH THUsman Ali AkbarÎncă nu există evaluări
- Anaemia in PregnancyDocument13 paginiAnaemia in PregnancyUsman Ali AkbarÎncă nu există evaluări
- IBS Pathophysiology & ManagementDocument18 paginiIBS Pathophysiology & ManagementUsman Ali AkbarÎncă nu există evaluări
- Ibs Presentation PDFDocument18 paginiIbs Presentation PDFUsman Ali AkbarÎncă nu există evaluări
- Clinical Calendar 2016-2018Document3 paginiClinical Calendar 2016-2018NickÎncă nu există evaluări
- Foreign Visiting Student Medical Status Form PDFDocument1 paginăForeign Visiting Student Medical Status Form PDFUsman Ali AkbarÎncă nu există evaluări
- Recurrent VomitingDocument16 paginiRecurrent VomitingUsman Ali AkbarÎncă nu există evaluări
- TSMEntry 2Document1 paginăTSMEntry 2Usman Ali AkbarÎncă nu există evaluări
- CORD PROLAPSE GUIDEDocument2 paginiCORD PROLAPSE GUIDEUsman Ali AkbarÎncă nu există evaluări
- Diseases of The StomachDocument17 paginiDiseases of The StomachUsman Ali AkbarÎncă nu există evaluări
- When Hope DiesDocument2 paginiWhen Hope DiesUsman Ali AkbarÎncă nu există evaluări
- Organophosphor US PoisoningDocument81 paginiOrganophosphor US PoisoningRamila MaharjanÎncă nu există evaluări
- Current Guidelines for Managing Organophosphorus PoisoningDocument6 paginiCurrent Guidelines for Managing Organophosphorus PoisoningSid DhayriÎncă nu există evaluări
- Pediatric Organophosphates Toxicity GuideDocument1 paginăPediatric Organophosphates Toxicity GuideJC HernándezÎncă nu există evaluări
- (Mantap) Slide Materi Anestesi Batch 3 2018Document74 pagini(Mantap) Slide Materi Anestesi Batch 3 2018Aditya PratamaÎncă nu există evaluări
- Dr. Ali's Uworld Notes For Step 2 CKDocument6 paginiDr. Ali's Uworld Notes For Step 2 CKuyesÎncă nu există evaluări
- PoisoningDocument39 paginiPoisoningNatnael ShifferawÎncă nu există evaluări
- MCQS ANS 01 Sol-1Document5 paginiMCQS ANS 01 Sol-1Samir Rekha Mukund JoshiÎncă nu există evaluări
- Pesticides Poisoning - Case Report: MedicineDocument5 paginiPesticides Poisoning - Case Report: MedicineKukuh KhumairoÎncă nu există evaluări
- Lesson Plan PoisoningDocument45 paginiLesson Plan PoisoningLoma Waghmare (Jadhav)100% (1)
- PHC 513: Pharmacology of Drugs Affecting the Peripheral Nervous SystemDocument19 paginiPHC 513: Pharmacology of Drugs Affecting the Peripheral Nervous SystemAimanRozlanÎncă nu există evaluări
- Organo & Paraquat PoisoningDocument54 paginiOrgano & Paraquat PoisoningNgu Ing SoonÎncă nu există evaluări
- Op Compound Poisoning Guidelines AapDocument6 paginiOp Compound Poisoning Guidelines AapchtbhtÎncă nu există evaluări
- ANS Pharmacology-Cholinergic AgentsDocument55 paginiANS Pharmacology-Cholinergic AgentsMarc Imhotep Cray, M.D.Încă nu există evaluări
- Organophosphate Poisoning ManagementDocument31 paginiOrganophosphate Poisoning ManagementLIDIYA MOL P VÎncă nu există evaluări
- KGD 2 IvanDocument92 paginiKGD 2 IvanrikarikaÎncă nu există evaluări
- Jan - AprDocument106 paginiJan - AprKickuÎncă nu există evaluări
- Organophosphateand Carbamatepoisoning: Andrew M. King,, Cynthia K. AaronDocument19 paginiOrganophosphateand Carbamatepoisoning: Andrew M. King,, Cynthia K. AaronGufront MustofaÎncă nu există evaluări
- Op PoisoningDocument13 paginiOp PoisoningDr-Jagadeesh MangamooriÎncă nu există evaluări
- Organophosphate PoisoningDocument40 paginiOrganophosphate PoisoningMadhu Sudhan PandeyaÎncă nu există evaluări
- Clinpharm SGD Organophosphayte PoisoningDocument2 paginiClinpharm SGD Organophosphayte PoisoningBea SamonteÎncă nu există evaluări
- Qdoc - Tips Topnotch Supplement Pharmacology HandoutDocument57 paginiQdoc - Tips Topnotch Supplement Pharmacology HandoutShehana MusahariÎncă nu există evaluări
- (Lakshman Karalliedde, Stanley Feldman, John HenryDocument510 pagini(Lakshman Karalliedde, Stanley Feldman, John HenryMeilaDwiputriÎncă nu există evaluări
- Organophosphorus PoisoningDocument15 paginiOrganophosphorus PoisoningtaufiAmaneeÎncă nu există evaluări
- Management of Acute Poisoning ANISH FINALDocument92 paginiManagement of Acute Poisoning ANISH FINALAnish JoshiÎncă nu există evaluări
- Predictors of Morbidities in Organophosphate PoisoningDocument17 paginiPredictors of Morbidities in Organophosphate PoisoningInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Organophosphate PoisoningDocument19 paginiOrganophosphate PoisoningapokawÎncă nu există evaluări
- QB Poisoning Final...Document31 paginiQB Poisoning Final...richard bolinaoÎncă nu există evaluări
- Mary Jancy Joy Et. AlDocument10 paginiMary Jancy Joy Et. AlSmith MpÎncă nu există evaluări
- Carbamate Poisoning - MSDDocument2 paginiCarbamate Poisoning - MSDAswin AÎncă nu există evaluări
- Acute Poisoning in Adults: Dr. S.P. Hewawasam MBBS, MDDocument76 paginiAcute Poisoning in Adults: Dr. S.P. Hewawasam MBBS, MDSamapriya Pasan Hewawasam100% (1)