S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Circulation and RespirationDocument18 paginiCirculation and Respirationmursidstone.mursidÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- EDIT Respiratory Failure Assessment and Problem SolvingDocument66 paginiEDIT Respiratory Failure Assessment and Problem Solvingmursidstone.mursidÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
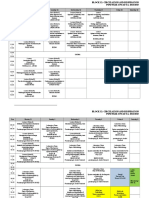
- Revisi Jadwal Blok 12 PK - 2015Document7 paginiRevisi Jadwal Blok 12 PK - 2015mursidstone.mursidÎncă nu există evaluări
- Anova Atp Basf Che Adenosine Trifosfat: Analysis of VariansDocument1 paginăAnova Atp Basf Che Adenosine Trifosfat: Analysis of Variansmursidstone.mursidÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Lampiran 2 Analisis Data Pengujian Distribusi Data: Case Processing SummaryDocument8 paginiLampiran 2 Analisis Data Pengujian Distribusi Data: Case Processing Summarymursidstone.mursidÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Recommendations For The Cardiovascular Screening of AthletesDocument8 paginiRecommendations For The Cardiovascular Screening of Athletesmursidstone.mursidÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Daftar Pustaka: Systematic Review. WHO. (Cited 2016 September 03) - Available FromDocument6 paginiDaftar Pustaka: Systematic Review. WHO. (Cited 2016 September 03) - Available Frommursidstone.mursidÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Analysis of Variance: LC: Lethal Concentration 50 LDDocument1 paginăAnalysis of Variance: LC: Lethal Concentration 50 LDmursidstone.mursidÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Aedes Sp. Analysis of Variance Baden Aniline and Soda FactoryDocument3 paginiAedes Sp. Analysis of Variance Baden Aniline and Soda Factorymursidstone.mursidÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Balai Litbang P2B2Document1 paginăBalai Litbang P2B2mursidstone.mursidÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Six Steps On Prescribing: Rustamaji/dr. Fian Faculty of Medicine Universitas Gadjah Mada/ Univ Tadulako 2016Document28 paginiSix Steps On Prescribing: Rustamaji/dr. Fian Faculty of Medicine Universitas Gadjah Mada/ Univ Tadulako 2016mursidstone.mursidÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Daftar Pustak1Document4 paginiDaftar Pustak1mursidstone.mursidÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Drug and Therapeutics Committee: Standard Treatment GuidelinesDocument26 paginiDrug and Therapeutics Committee: Standard Treatment Guidelinesmursidstone.mursidÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- First Page PDFDocument1 paginăFirst Page PDFJordan BzÎncă nu există evaluări
- Congenital HerniaDocument5 paginiCongenital HerniaBlazxy EyreÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- MCQ Tyba Abnormal Psychology 2020Document16 paginiMCQ Tyba Abnormal Psychology 2020phanishashidharÎncă nu există evaluări
- 68W Medic Guide IDocument8 pagini68W Medic Guide Ijonwick100% (6)
- PathogenesisDocument14 paginiPathogenesisIdreesÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Breastfeeding Tsek AdvocacyDocument81 paginiBreastfeeding Tsek AdvocacyBelle A. Basilio100% (3)
- Geriatrics RehabDocument30 paginiGeriatrics RehabNasroon BhambhaniÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Bsped Dka Guidelines 2020Document23 paginiBsped Dka Guidelines 2020drsaleemÎncă nu există evaluări
- Bone Infections - Acute OsteomyelitisDocument35 paginiBone Infections - Acute Osteomyelitismeto40% (5)
- Pengaruh Kompresi RJP Dengan Metronom Terhadap Kualitas Kompresi RJP Yang Dilakukan Mahasiswa PerawatDocument7 paginiPengaruh Kompresi RJP Dengan Metronom Terhadap Kualitas Kompresi RJP Yang Dilakukan Mahasiswa PerawatGabriela Adeleda LeiwakabessyÎncă nu există evaluări
- Augmentin Tablet Pi Ipi13 SiDocument11 paginiAugmentin Tablet Pi Ipi13 Siاسد راجÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Preventing Hip Dysplasia BrochureDocument2 paginiPreventing Hip Dysplasia Brochurepcr_22Încă nu există evaluări
- Optimal Management of Collagenous Colitis A Review 021016Document9 paginiOptimal Management of Collagenous Colitis A Review 021016Eliza DNÎncă nu există evaluări
- First Aid Kits & Their ImportanceDocument25 paginiFirst Aid Kits & Their ImportanceJennette BelliotÎncă nu există evaluări
- CH 32 Gallbladder and Extrahepatic Biliary SystemDocument33 paginiCH 32 Gallbladder and Extrahepatic Biliary SystemElisha BernabeÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Dizziness HXDocument4 paginiDizziness HXbadmanÎncă nu există evaluări
- Hepatitis B: What Is It?Document2 paginiHepatitis B: What Is It?DrBertram ForerÎncă nu există evaluări
- Ijcem0006 0358Document9 paginiIjcem0006 0358najwaÎncă nu există evaluări
- Head TraumaDocument4 paginiHead TraumaDaniel GeduquioÎncă nu există evaluări
- Informative Speech Outline Group 3Document4 paginiInformative Speech Outline Group 3Princee RaaidÎncă nu există evaluări
- Orofacial Pain Speciality ApplicationDocument329 paginiOrofacial Pain Speciality ApplicationOromax OhmRajaniÎncă nu există evaluări
- Facial Diagnosis Cell Salt IntroductionDocument15 paginiFacial Diagnosis Cell Salt IntroductionRalucaFlorentina100% (3)
- Laryngopharyngeal Reflux and Functional Laryngeal Disorder: Perspective and Common Practice of The General GastroenterologistDocument9 paginiLaryngopharyngeal Reflux and Functional Laryngeal Disorder: Perspective and Common Practice of The General GastroenterologistKenzi A HasyaputraÎncă nu există evaluări
- Health: Deepen: Vitex Negundo or Lagundi (Dangla)Document1 paginăHealth: Deepen: Vitex Negundo or Lagundi (Dangla)Jio RillorazaÎncă nu există evaluări
- NCRP Report No. 177 PDFDocument245 paginiNCRP Report No. 177 PDFVivien FerradaÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- DR - Iniesta ReportDocument97 paginiDR - Iniesta ReportRaceRadioÎncă nu există evaluări
- Meconium-Stained Amniotic Fluid MSAFDocument54 paginiMeconium-Stained Amniotic Fluid MSAFJhansi PeddiÎncă nu există evaluări
- Cycles and Cycle Safety: Pegasus PharmaceuticalsDocument25 paginiCycles and Cycle Safety: Pegasus PharmaceuticalsMahmoud El Mohamdy100% (2)
- General Surgery ConceptsDocument4 paginiGeneral Surgery ConceptsPau De GuzmanÎncă nu există evaluări
- Vein Artery Capillary: Thin Wall Wide Lumen Valve Thick Wall Narrow Lumen One Cell Thick WallDocument1 paginăVein Artery Capillary: Thin Wall Wide Lumen Valve Thick Wall Narrow Lumen One Cell Thick WallHuiso RohÎncă nu există evaluări