S-ar putea să vă placă și
- Neurological Health AssessmentDocument55 paginiNeurological Health Assessment09-bays-rhythmsÎncă nu există evaluări
- Total Reflexology: The Reflex Points for Physical, Emotional, and Psychological HealingDe la EverandTotal Reflexology: The Reflex Points for Physical, Emotional, and Psychological HealingEvaluare: 2.5 din 5 stele2.5/5 (2)
- Practical Neurology: Neurologic ExamDocument114 paginiPractical Neurology: Neurologic ExamDannyÎncă nu există evaluări
- The Neurological Exam Made SimpleDocument49 paginiThe Neurological Exam Made SimpleRizki AmaliahÎncă nu există evaluări
- The Neurological ExaminationDocument53 paginiThe Neurological ExaminationApolinar González Hernández100% (2)
- Clinical Localization and History in NeurologyDocument41 paginiClinical Localization and History in NeurologyRhomizal MazaliÎncă nu există evaluări
- Neurology: by Dennis Jason Alcantara, RN, USRN, MAN CanDocument213 paginiNeurology: by Dennis Jason Alcantara, RN, USRN, MAN CanKristel-Mia Dimalanta RamosÎncă nu există evaluări
- Erman Fandialan M.D. Department of Clinical Neurosciences UermmmcDocument48 paginiErman Fandialan M.D. Department of Clinical Neurosciences Uermmmclovelots1234100% (1)
- Care of Clients With Problems Related To Neurological SystemDocument44 paginiCare of Clients With Problems Related To Neurological Systemapi-3735995100% (1)
- Introduction To Clinical Neurology - 2018Document68 paginiIntroduction To Clinical Neurology - 2018Alberto MayorgaÎncă nu există evaluări
- Neurologic Examination English Class2011 1Document79 paginiNeurologic Examination English Class2011 1HieLdaJanuariaÎncă nu există evaluări
- Sub - Medical Surgical Nursing: Assignment On Neurological AssessmentDocument11 paginiSub - Medical Surgical Nursing: Assignment On Neurological Assessmentkamini Choudhary100% (1)
- Neurologic ExaminationDocument67 paginiNeurologic Examinationሀይደር ዶ.ር100% (1)
- Neurological Health AssessmentDocument63 paginiNeurological Health AssessmentAhmed ElryahÎncă nu există evaluări
- Neurological Examination 3Document46 paginiNeurological Examination 3VIKAS PUNIAÎncă nu există evaluări
- Neuroanatomy & Neuropsychiatric Aspects of Frontal LobeDocument56 paginiNeuroanatomy & Neuropsychiatric Aspects of Frontal LobeShabaz AkhtarÎncă nu există evaluări
- Approach To Neurological EmergenciesMAY2013Document69 paginiApproach To Neurological EmergenciesMAY2013PhaimÎncă nu există evaluări
- LocalizationDocument38 paginiLocalizationWilson HannahÎncă nu există evaluări
- 7-Nervous SystemDocument30 pagini7-Nervous SystemStephen Yao AddoÎncă nu există evaluări
- Introductory Lecture, Neurological Examination: General OverviewDocument8 paginiIntroductory Lecture, Neurological Examination: General OverviewmustafaÎncă nu există evaluări
- KKD Cranial NDocument23 paginiKKD Cranial NAdie Kristanto100% (1)
- 206 Neuro Fall 2015Document89 pagini206 Neuro Fall 2015baasheÎncă nu există evaluări
- Neuro 2Document41 paginiNeuro 2Cosmina CorbeanuÎncă nu există evaluări
- NaveedDocument18 paginiNaveednaveed aliÎncă nu există evaluări
- Neurologic Examination: Muhammad Iqbal BasriDocument79 paginiNeurologic Examination: Muhammad Iqbal Basribima sarewoÎncă nu există evaluări
- Cranial Nerve Examination 341Document29 paginiCranial Nerve Examination 341Chanu HandaÎncă nu există evaluări
- Responses To Altered PerceptionDocument74 paginiResponses To Altered PerceptionANDREA JUSTINE CARDEÑOÎncă nu există evaluări
- Neuro Examination (Auto-Saved)Document18 paginiNeuro Examination (Auto-Saved)MALIK WASEEM ABBASÎncă nu există evaluări
- Cranial NervesDocument48 paginiCranial NervesdericÎncă nu există evaluări
- Anamnesis Dan Diagnosis Topis (Dr. Hendro SP.S)Document27 paginiAnamnesis Dan Diagnosis Topis (Dr. Hendro SP.S)PatrickNicholsÎncă nu există evaluări
- CP6 - 6 - Neurological System P2Document44 paginiCP6 - 6 - Neurological System P2dafabc50Încă nu există evaluări
- Neurology Gaye McCaffertyDocument28 paginiNeurology Gaye McCaffertyKrishna KanthÎncă nu există evaluări
- Obcl 1 Week 16 Perception and CoordinationDocument20 paginiObcl 1 Week 16 Perception and CoordinationMichelle Mallare100% (1)
- Nervous System Examination SynopsisDocument26 paginiNervous System Examination Synopsisaarti chandeÎncă nu există evaluări
- Neurology ExaminationDocument31 paginiNeurology ExaminationEtana AdamÎncă nu există evaluări
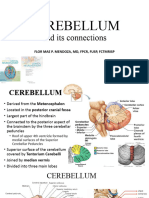
- CerebellumDocument32 paginiCerebellumDr VirenÎncă nu există evaluări
- Neurological Assessment and Examination 1Document35 paginiNeurological Assessment and Examination 1Esmareldah Henry SirueÎncă nu există evaluări
- CerebellumDocument49 paginiCerebellumsjs6r8wwv9Încă nu există evaluări
- Nervous SystemDocument10 paginiNervous Systemshenric16Încă nu există evaluări
- Paediatrics ClinicalsDocument84 paginiPaediatrics ClinicalsJeevan VijayÎncă nu există evaluări
- CNS Examination: Done by DR/ Abdullah Mohd. Jan MBBS, InternDocument37 paginiCNS Examination: Done by DR/ Abdullah Mohd. Jan MBBS, InternBrajesh MouryaÎncă nu există evaluări
- Nervous System For NursingDocument112 paginiNervous System For Nursingamaracha2003100% (1)
- 4-TOPICAL DIAGNOSIS-clinical AnatomyDocument61 pagini4-TOPICAL DIAGNOSIS-clinical AnatomyMuhammad SyauqadÎncă nu există evaluări
- 1cranial NervesDocument48 pagini1cranial NervesKaarthigan RamaiahÎncă nu există evaluări
- Nerve ExamsDocument18 paginiNerve Examszulaikhaa.bbÎncă nu există evaluări
- Neuro Lecture NotesDocument41 paginiNeuro Lecture Notescziel23Încă nu există evaluări
- Ataxia: Pediatric Neurology Quick TalksDocument18 paginiAtaxia: Pediatric Neurology Quick TalksAlex GasnasÎncă nu există evaluări
- Introduction To Physical Diagnosis:: NeurologyDocument24 paginiIntroduction To Physical Diagnosis:: NeurologyGraceÎncă nu există evaluări
- Cns Examination: BY Chris VictorDocument35 paginiCns Examination: BY Chris VictorRwabugili ChrisÎncă nu există evaluări
- Neuorlogical AssessmentDocument41 paginiNeuorlogical AssessmentSalman KhanÎncă nu există evaluări
- Cranial Nerve 6, 7 and 8 (Short Presentation)Document33 paginiCranial Nerve 6, 7 and 8 (Short Presentation)3uvpÎncă nu există evaluări
- Examination of Nervous SystemDocument25 paginiExamination of Nervous SystemASAP teleÎncă nu există evaluări
- Nurologic Ass Faculty - 2023 1st Term-1Document29 paginiNurologic Ass Faculty - 2023 1st Term-1cwley64Încă nu există evaluări
- Neurological AssessmentDocument76 paginiNeurological Assessmentjcabatit3Încă nu există evaluări
- CP Case PreDocument35 paginiCP Case PreCatherine CarmonaÎncă nu există evaluări
- Neurological ExaminationDocument71 paginiNeurological ExaminationAmbreen SabaÎncă nu există evaluări
- Cerebral PalsyDocument21 paginiCerebral PalsyEMily AbastaÎncă nu există evaluări
- Neurological AssessmentDocument34 paginiNeurological Assessmentdrprasant100% (9)
- Happy Birthday SongDocument1 paginăHappy Birthday SongPratama Aditya BiantoroÎncă nu există evaluări
- Practice Essentials: Essential Update: New Guidelines From KDIGODocument13 paginiPractice Essentials: Essential Update: New Guidelines From KDIGOPratama Aditya BiantoroÎncă nu există evaluări
- Selection of Proper Antiepileptic Drugs: 1 IntroductionDocument1 paginăSelection of Proper Antiepileptic Drugs: 1 IntroductionPratama Aditya BiantoroÎncă nu există evaluări
- Cocaine Use and StrokeDocument7 paginiCocaine Use and StrokePratama Aditya BiantoroÎncă nu există evaluări