S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- IMS Oncology Trend Report 2017 Advances Complexity CostDocument47 paginiIMS Oncology Trend Report 2017 Advances Complexity CostEkta Dhawan RampalÎncă nu există evaluări
- Anticancer Drugs Final PDFDocument8 paginiAnticancer Drugs Final PDFAisha Jamil100% (1)
- Brosuri Chimioterapie Update 2020 673 PDFDocument282 paginiBrosuri Chimioterapie Update 2020 673 PDFAnna Dumitrache67% (3)
- Adjuvant Therapy in Breast CancerDocument21 paginiAdjuvant Therapy in Breast CancerHassan.shehriÎncă nu există evaluări
- Role of High Dose Methotrexate in Osteosarcoma - FinalDocument30 paginiRole of High Dose Methotrexate in Osteosarcoma - FinalHemanth KumarÎncă nu există evaluări
- CINV Guidelines PDFDocument8 paginiCINV Guidelines PDFagilÎncă nu există evaluări
- Basic Principle of ChemotherapyDocument29 paginiBasic Principle of ChemotherapyDevby Ulfandi100% (1)
- BB Cancer A To KDocument49 paginiBB Cancer A To KWaris TriyonoÎncă nu există evaluări
- Extravasation Neutral (Non-Irritant) Irritant Irritant With Vesicant Properties VesicantsDocument12 paginiExtravasation Neutral (Non-Irritant) Irritant Irritant With Vesicant Properties VesicantsmarcÎncă nu există evaluări
- The Top 20 Drugs by Worldwide Sales in 2020 - Fierce PharmaDocument50 paginiThe Top 20 Drugs by Worldwide Sales in 2020 - Fierce PharmaBonnie DebbarmaÎncă nu există evaluări
- Anti EmesisDocument62 paginiAnti EmesisFelipe Esteban Albornoz CancinoÎncă nu există evaluări
- Therapeutic Monoclonal Antibodies Approved by FDA in 2019 (Mini Review)Document2 paginiTherapeutic Monoclonal Antibodies Approved by FDA in 2019 (Mini Review)asclepiuspdfsÎncă nu există evaluări
- Chemo DrugsDocument4 paginiChemo DrugsFidel SantongÎncă nu există evaluări
- Cyclophosphamide (Cyclovid) - Epirubicin - VincristineDocument1 paginăCyclophosphamide (Cyclovid) - Epirubicin - VincristineEma Ratna KartinawatiÎncă nu există evaluări
- Antineoplastic AgentsDocument25 paginiAntineoplastic AgentsAlyssaGrandeMontimorÎncă nu există evaluări
- ClotrimazoleDocument2 paginiClotrimazoleSagar GuptaÎncă nu există evaluări
- Inventario Oncologicos AgostoDocument4 paginiInventario Oncologicos AgostoAdeliana USECHE SUAREZÎncă nu există evaluări
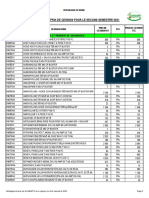
- Catalogue de Prix de Cession Pour Le Second Semestre 2021Document10 paginiCatalogue de Prix de Cession Pour Le Second Semestre 2021Mr BATTAHÎncă nu există evaluări
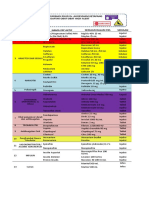
- High Alert List (Sheet2) - Lampiran Drs Masrial MDocument13 paginiHigh Alert List (Sheet2) - Lampiran Drs Masrial MDini RahmaÎncă nu există evaluări
- Chiara Leo Canine Lymphoma TherapyDocument18 paginiChiara Leo Canine Lymphoma TherapyCabinet VeterinarÎncă nu există evaluări
- Oncology Products ListDocument4 paginiOncology Products ListSUBHASHÎncă nu există evaluări
- ChemotherapyDocument1 paginăChemotherapyGerardLum100% (2)
- WRHA Drug List - Feb'16 CYTOTOXIC LISTDocument2 paginiWRHA Drug List - Feb'16 CYTOTOXIC LISTOlinÎncă nu există evaluări
- Bodeguita FarmaceuticaDocument20 paginiBodeguita FarmaceuticaDavid CoelloÎncă nu există evaluări
- Anticancer Pharmacology: D. Lyrawati, Apt. MS., PHDDocument52 paginiAnticancer Pharmacology: D. Lyrawati, Apt. MS., PHDSiti Jannatul HusnahÎncă nu există evaluări
- Diluent RateDocument3 paginiDiluent RateMohamed Abdel-AzizÎncă nu există evaluări
- RFQ Medicine 20170523Document16 paginiRFQ Medicine 20170523Vijay BarreyÎncă nu există evaluări
- Catalogo General - PharmacoDocument27 paginiCatalogo General - PharmacomauventuragÎncă nu există evaluări
- Protocol Outline Remission Induction (6-7 Weeks)Document3 paginiProtocol Outline Remission Induction (6-7 Weeks)Mohammed HaiderÎncă nu există evaluări
- Global Rheumatoid Arthritis Drugs MarketDocument2 paginiGlobal Rheumatoid Arthritis Drugs MarketiHealthcareAnalyst, Inc.Încă nu există evaluări