S-ar putea să vă placă și
- 15 AminesDocument66 pagini15 AminesHamid Hussain HamidÎncă nu există evaluări
- ArrhythmiasDocument26 paginiArrhythmiasHamid Hussain HamidÎncă nu există evaluări
- 03 Organic Chemistry Introduction 2Document126 pagini03 Organic Chemistry Introduction 2Hamid Hussain HamidÎncă nu există evaluări
- 01 Aromatic Hydrocarbons BenzeneDocument116 pagini01 Aromatic Hydrocarbons BenzeneHamid Hussain HamidÎncă nu există evaluări
- Physiology of Smell and Taste-MyDocument46 paginiPhysiology of Smell and Taste-MyHamid Hussain HamidÎncă nu există evaluări
- Nuclear Magnetic Resonance SpectrosDocument167 paginiNuclear Magnetic Resonance SpectrosHamid Hussain HamidÎncă nu există evaluări
- 17 EthersDocument38 pagini17 EthersHamid Hussain HamidÎncă nu există evaluări
- 20 Reaction of AlcoholsDocument18 pagini20 Reaction of AlcoholsHamid Hussain HamidÎncă nu există evaluări
- Top 300 Drugs PDFDocument31 paginiTop 300 Drugs PDFVin Bitz100% (1)
- Infrared SpectrosDocument139 paginiInfrared SpectrosHamid Hussain Hamid100% (1)
- 02 AlkylhalidesDocument78 pagini02 AlkylhalidesHamid Hussain HamidÎncă nu există evaluări
- General Anesthetics AgentsDocument42 paginiGeneral Anesthetics AgentsHamid Hussain HamidÎncă nu există evaluări
- 08 Alkenes Structure and ReactivityDocument58 pagini08 Alkenes Structure and ReactivityHamid Hussain HamidÎncă nu există evaluări
- 09 Alkene Synthesis and Electrophilic AdditionDocument59 pagini09 Alkene Synthesis and Electrophilic AdditionHamid Hussain HamidÎncă nu există evaluări
- Mass SpectrometryADocument186 paginiMass SpectrometryAHamid Hussain HamidÎncă nu există evaluări
- Using 1 H NMR Spectroscopy For Structure DeterminationDocument24 paginiUsing 1 H NMR Spectroscopy For Structure DeterminationHamid Hussain HamidÎncă nu există evaluări
- 6-Drugs Acting On The Renal System - 2Document65 pagini6-Drugs Acting On The Renal System - 2Hamid Hussain HamidÎncă nu există evaluări
- Microbiology 1 To 6 Semster 8 SterilizationDocument8 paginiMicrobiology 1 To 6 Semster 8 SterilizationHamid Hussain HamidÎncă nu există evaluări
- 2 CNS Sys PharmacologyDocument75 pagini2 CNS Sys PharmacologyHamid Hussain HamidÎncă nu există evaluări
- 4-Sympathomimetid Drugs Aa4Document81 pagini4-Sympathomimetid Drugs Aa4Hamid Hussain HamidÎncă nu există evaluări
- Core of Medical Physiology 2 Ed3 PDFDocument442 paginiCore of Medical Physiology 2 Ed3 PDFHamid Hussain Hamid94% (17)
- Autonomic Mcqs ExplainedDocument7 paginiAutonomic Mcqs ExplainedHamid Hussain HamidÎncă nu există evaluări
- 3 Cholinergic BlockersDocument37 pagini3 Cholinergic BlockersHamid Hussain HamidÎncă nu există evaluări
- 1 Autonomic Introduction (Excellent)Document70 pagini1 Autonomic Introduction (Excellent)Hamid Hussain HamidÎncă nu există evaluări
- 2 - ParasympathomimeticsDocument99 pagini2 - ParasympathomimeticsHamid Hussain HamidÎncă nu există evaluări
- 7a - Antihistamine 09Document37 pagini7a - Antihistamine 09Hamid Hussain HamidÎncă nu există evaluări
- 8 Vasoactive PeptidesDocument49 pagini8 Vasoactive PeptidesHamid Hussain HamidÎncă nu există evaluări
- 7c Ergot AlkaloidsDocument11 pagini7c Ergot AlkaloidsHamid Hussain HamidÎncă nu există evaluări
- 5 Adrenoceptor BlockersDocument52 pagini5 Adrenoceptor BlockersHamid Hussain HamidÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Orange BookDocument70 paginiOrange BookAIMANIBRAHIM82Încă nu există evaluări
- Eye drops, creams and ointments price listDocument2 paginiEye drops, creams and ointments price listSella SylviaÎncă nu există evaluări
- Description of Drug Information Service (PIO) of Pharmacy Study Program, Atma Jaya Catholic University of Indonesia During Covid-19 Pandemic Period of April - July 2020Document8 paginiDescription of Drug Information Service (PIO) of Pharmacy Study Program, Atma Jaya Catholic University of Indonesia During Covid-19 Pandemic Period of April - July 2020Ina SuciÎncă nu există evaluări
- Impact of Globalization of Pharmaceutical IndustriesDocument7 paginiImpact of Globalization of Pharmaceutical IndustriesAbhishek PrakashÎncă nu există evaluări
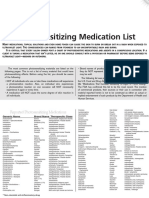
- Photosensitizing Medication ListDocument3 paginiPhotosensitizing Medication ListDimas RfÎncă nu există evaluări
- Learning Materials and Students WorksheetDocument3 paginiLearning Materials and Students WorksheetRatu Rini NurhayatiÎncă nu există evaluări
- List of Medicines with DetailsDocument1 paginăList of Medicines with Detailsevi zaqiyahÎncă nu există evaluări
- Canada Drugs Direct PAFDocument1 paginăCanada Drugs Direct PAFrjohngdcÎncă nu există evaluări
- LDN Fact Sheet Provides Dosing and Mechanism DetailsDocument8 paginiLDN Fact Sheet Provides Dosing and Mechanism DetailscristiÎncă nu există evaluări
- Ceiling-Price-List-F 30 Sep 2020Document21 paginiCeiling-Price-List-F 30 Sep 2020nagashayana gÎncă nu există evaluări
- Procure APIs Simply and Cost-Effectively with TiefenbacherDocument16 paginiProcure APIs Simply and Cost-Effectively with Tiefenbacherমোঃ এমদাদুল হকÎncă nu există evaluări
- Medication Management GuideDocument52 paginiMedication Management Guideyuhuma_qyu6841100% (1)
- Ezetimibe An Overeview of Analytical Methods For The Drug SubstanceDocument6 paginiEzetimibe An Overeview of Analytical Methods For The Drug SubstanceEditor IJTSRDÎncă nu există evaluări
- Produttori AzitroDocument10 paginiProduttori AzitroMario MicciarelliÎncă nu există evaluări
- Phentermine 37.5 MGDocument4 paginiPhentermine 37.5 MGMichealÎncă nu există evaluări
- Laporan Perawat Imcu t6 LT 2 Update 260421 Google DriveDocument46 paginiLaporan Perawat Imcu t6 LT 2 Update 260421 Google DriveNurse HandsomeÎncă nu există evaluări
- Μ. Bs Eb‡Qi Bvg †Jl‡Ki Bvg Cyivzb B¤^I Eb‡Qi Lð Eb Msl¨V G~J¨ MöæcDocument121 paginiΜ. Bs Eb‡Qi Bvg †Jl‡Ki Bvg Cyivzb B¤^I Eb‡Qi Lð Eb Msl¨V G~J¨ MöæcErshad RoufÎncă nu există evaluări
- A Comparative Evaluation of Furosemide Tablets Marketed in LibyaDocument7 paginiA Comparative Evaluation of Furosemide Tablets Marketed in LibyaMediterr J Pharm Pharm SciÎncă nu există evaluări
- 10 Rules For Safer Drug UseDocument4 pagini10 Rules For Safer Drug UseBenjel AndayaÎncă nu există evaluări
- Pharmarocks Pre-Gpat Mock Test-13Document13 paginiPharmarocks Pre-Gpat Mock Test-13Subhodeep Sengupta67% (3)
- Pharmaceutical Calc ExamDocument15 paginiPharmaceutical Calc ExamMickey Brown100% (2)
- Bawalan, Hewlett Pearl L. February 11, 2021 Module 4: AsthmaDocument5 paginiBawalan, Hewlett Pearl L. February 11, 2021 Module 4: AsthmaHewlett Pearl BawalanÎncă nu există evaluări
- Introduction To Toxicology 2017 by Dr. PerezDocument15 paginiIntroduction To Toxicology 2017 by Dr. PerezJohn Christopher LucesÎncă nu există evaluări
- Antifungal ClassDocument25 paginiAntifungal ClassRifa AudinaÎncă nu există evaluări
- Chemistry Research Journal, 2018, 3 (2) :135-140Document6 paginiChemistry Research Journal, 2018, 3 (2) :135-140NeerajKumarÎncă nu există evaluări
- Dosage Titration PresentationDocument17 paginiDosage Titration PresentationNursyNurseÎncă nu există evaluări
- Pharmaceutical AnalysisDocument73 paginiPharmaceutical AnalysisChristinaÎncă nu există evaluări
- Regulatory Perspectives On Strength-Dependent Dissolution ProfilesDocument11 paginiRegulatory Perspectives On Strength-Dependent Dissolution ProfilesJminsÎncă nu există evaluări
- HAAD Exam 06-08-2020Document16 paginiHAAD Exam 06-08-2020Sandeep Kanneganti100% (2)
- Ampicillin SulbactamDocument3 paginiAmpicillin Sulbactamrhon_123rd88% (17)