S-ar putea să vă placă și
- Chikungunya WDocument11 paginiChikungunya Wapi-378136896100% (1)
- Arboviruses: R.Varidianto Yudo T., Dr.,MkesDocument19 paginiArboviruses: R.Varidianto Yudo T., Dr.,MkesalbertmogÎncă nu există evaluări
- Rhabdoviruses - Teaching RabiesDocument70 paginiRhabdoviruses - Teaching Rabiestummalapalli venkateswara raoÎncă nu există evaluări
- CephalosporinsDocument21 paginiCephalosporinsMoha Bin Ladiif75% (4)
- Arthropod-Borne Viruses Part OneDocument80 paginiArthropod-Borne Viruses Part Onetummalapalli venkateswara rao100% (1)
- Peniciline: Dr. Md. Rageeb Md. Usman Associate Professor Department of PharmacognosyDocument9 paginiPeniciline: Dr. Md. Rageeb Md. Usman Associate Professor Department of PharmacognosyAnonymous TCbZigVqÎncă nu există evaluări
- 24 05 2021 Floroquinolones DR - Syeda ZainDocument46 pagini24 05 2021 Floroquinolones DR - Syeda ZaintehreemÎncă nu există evaluări
- FluroquinolonesDocument29 paginiFluroquinolonestummalapalli venkateswara rao0% (1)
- Rickettsia Coxiella: Prof. Khalifa Sifaw GhengheshDocument20 paginiRickettsia Coxiella: Prof. Khalifa Sifaw GhengheshKhalifa Sifaw GhengheshÎncă nu există evaluări
- Brucellosis: A Highly Contagious Zoonotic DiseaseDocument55 paginiBrucellosis: A Highly Contagious Zoonotic Diseasesana shakeelÎncă nu există evaluări
- Gilut Herpes ZosteRDocument24 paginiGilut Herpes ZosteRdimasahadiantoÎncă nu există evaluări
- Cutaneous Leishmaniasis: Caused by A Protozoa Called Leishmania PathogenesisDocument30 paginiCutaneous Leishmaniasis: Caused by A Protozoa Called Leishmania PathogenesisHudh HudÎncă nu există evaluări
- Spirochetes: Aashutosh Nama M.SC Microbiology Sem - 1 Dr. B Lal Institute of BiotechnologyDocument34 paginiSpirochetes: Aashutosh Nama M.SC Microbiology Sem - 1 Dr. B Lal Institute of Biotechnologyaashutosh namaÎncă nu există evaluări
- Rat Bite FeversDocument23 paginiRat Bite Feverstummalapalli venkateswara raoÎncă nu există evaluări
- Pseudomonas An UpdateDocument82 paginiPseudomonas An Updatetummalapalli venkateswara raoÎncă nu există evaluări
- Influenza: DR.T .V.R Ao MDDocument81 paginiInfluenza: DR.T .V.R Ao MDtummalapalli venkateswara raoÎncă nu există evaluări
- Elizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDDocument28 paginiElizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDtummalapalli venkateswara raoÎncă nu există evaluări
- Lecture 1 - InfluenzaDocument67 paginiLecture 1 - InfluenzaShaimaa AbdulkadirÎncă nu există evaluări
- MUMPS AND INFLUENZA: CAUSES, SYMPTOMS AND PREVENTIONDocument15 paginiMUMPS AND INFLUENZA: CAUSES, SYMPTOMS AND PREVENTIONNeethu Mariya MathewÎncă nu există evaluări
- Actinomyces & Nocardia 06-07-MedDocument11 paginiActinomyces & Nocardia 06-07-Medapi-3699361Încă nu există evaluări
- Infectious Diseases of The HeartDocument84 paginiInfectious Diseases of The HeartHarold DiasanaÎncă nu există evaluări
- Meningitis In Children: Signs, Symptoms And TreatmentDocument48 paginiMeningitis In Children: Signs, Symptoms And TreatmentAli FalihÎncă nu există evaluări
- 11 Spirochetes 130520112830 Phpapp02Document61 pagini11 Spirochetes 130520112830 Phpapp02Manisanthosh KumarÎncă nu există evaluări
- Understanding Chlamydiae InfectionsDocument32 paginiUnderstanding Chlamydiae InfectionsNaing Lin SoeÎncă nu există evaluări
- Severe Acute Respiratory Syndrome: (Sars)Document16 paginiSevere Acute Respiratory Syndrome: (Sars)tummalapalli venkateswara raoÎncă nu există evaluări
- SAR TetracyclinesDocument24 paginiSAR TetracyclinesEspañola Eloise100% (1)
- Melioidosis.: Burkholderia PseudomalleiDocument34 paginiMelioidosis.: Burkholderia Pseudomalleitummalapalli venkateswara raoÎncă nu există evaluări
- Ebola Virus Disease: I. Signs and SymptomsDocument8 paginiEbola Virus Disease: I. Signs and SymptomsBoy BoyÎncă nu există evaluări
- What is rubella? Causes, symptoms, and prevention of German measlesDocument9 paginiWhat is rubella? Causes, symptoms, and prevention of German measlesMd A RAZZAKÎncă nu există evaluări
- Infections in Pregnancy FinalDocument67 paginiInfections in Pregnancy FinalkashafÎncă nu există evaluări
- HOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDDocument61 paginiHOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDtummalapalli venkateswara raoÎncă nu există evaluări
- Propagation of Lyophilised BacteriaDocument2 paginiPropagation of Lyophilised Bacteriatummalapalli venkateswara raoÎncă nu există evaluări
- Swine Flu Pandemic GuideDocument57 paginiSwine Flu Pandemic GuidemlbonthelineÎncă nu există evaluări
- Arthropod Borne InfectionsDocument135 paginiArthropod Borne InfectionspthamainiÎncă nu există evaluări
- Clinical History and Examination of Patients With Infectious DiseaseDocument43 paginiClinical History and Examination of Patients With Infectious DiseaseMarc Imhotep Cray, M.D.Încă nu există evaluări
- Shankland NHL Lancet Review PDFDocument10 paginiShankland NHL Lancet Review PDFNadhila ByantÎncă nu există evaluări
- Tuberculosis Lecture 1Document34 paginiTuberculosis Lecture 1Samson SeiduÎncă nu există evaluări
- Clinical Bacteriology: Fawad Mahmood M.Phil. Medical Laboratory SciencesDocument8 paginiClinical Bacteriology: Fawad Mahmood M.Phil. Medical Laboratory SciencesFawad SawabiÎncă nu există evaluări
- Malaria FalciparumDocument35 paginiMalaria FalciparumAboubakar Moalim Mahad moh'dÎncă nu există evaluări
- Neurological Manifestations of HIV/AIDSDocument34 paginiNeurological Manifestations of HIV/AIDSashuÎncă nu există evaluări
- Peptic UlcerDocument31 paginiPeptic UlcerHarpal Bajwa0% (1)
- Classic Childhood ExanthemsDocument66 paginiClassic Childhood ExanthemsBorzoo Tajdin100% (1)
- Fever With Rash SeminarDocument98 paginiFever With Rash SeminarSYAZRIANA SUHAIMIÎncă nu există evaluări
- Case 10 Hiv-AidsDocument47 paginiCase 10 Hiv-AidsErikah Eirah BeloriaÎncă nu există evaluări
- Virology NotesDocument81 paginiVirology NotesraulÎncă nu există evaluări
- Viral Hemorrhagic FeverDocument44 paginiViral Hemorrhagic Feverega100% (1)
- Chapter 65 (Introduction To Viruses)Document16 paginiChapter 65 (Introduction To Viruses)leoÎncă nu există evaluări
- HepatitisDocument65 paginiHepatitisgali3033Încă nu există evaluări
- Cestode SDocument38 paginiCestode SJang JangÎncă nu există evaluări
- Malaria 25 03 09Document131 paginiMalaria 25 03 09Dr.Jagadish Nuchina100% (5)
- ElephantiasisDocument23 paginiElephantiasisNitin0% (1)
- Tyhpoid FeverDocument6 paginiTyhpoid FeverMade Oka Heryana100% (1)
- Congenital Viral InfectionsDocument43 paginiCongenital Viral Infectionsannie1970100% (1)
- Hiv PPDocument37 paginiHiv PPJitendra YadavÎncă nu există evaluări
- Myiasis and Strike: Dr. Thahsin Farjana Associate Professor Dept. of Parasitology BAUDocument33 paginiMyiasis and Strike: Dr. Thahsin Farjana Associate Professor Dept. of Parasitology BAUChuramoni Saha100% (1)
- (Human Immunodeficiency Virus) &: Acquired Immune Deficiency SyndromeDocument61 pagini(Human Immunodeficiency Virus) &: Acquired Immune Deficiency SyndromeGufron MustofaÎncă nu există evaluări
- SpirochaetesDocument31 paginiSpirochaetesblue_blooded23Încă nu există evaluări
- 24.11.09 PPT On Intrauterine InfectionDocument57 pagini24.11.09 PPT On Intrauterine InfectionDhara Meena90% (10)
- Trichomoniasis: T. Vaginalis Is A Parasitic Protozoan, and The Taxonomic Position Is Based On The ClassificationDocument15 paginiTrichomoniasis: T. Vaginalis Is A Parasitic Protozoan, and The Taxonomic Position Is Based On The Classificationrave robÎncă nu există evaluări
- Tropmed Lecture 4Document78 paginiTropmed Lecture 4VerarisnaÎncă nu există evaluări
- Disorders of The Wihte CellsDocument22 paginiDisorders of The Wihte CellsVerarisnaÎncă nu există evaluări
- Disorders of The Wihte CellsDocument22 paginiDisorders of The Wihte CellsVerarisnaÎncă nu există evaluări
- Hepatology: An Introduction to Viral HepatitisDocument50 paginiHepatology: An Introduction to Viral HepatitisDwi WulandariÎncă nu există evaluări
- Hepatology: An Introduction to Viral HepatitisDocument50 paginiHepatology: An Introduction to Viral HepatitisDwi WulandariÎncă nu există evaluări
- Tropical Infection DiseasesDocument59 paginiTropical Infection DiseasesVerarisnaÎncă nu există evaluări
- Tropical Infection DiseasesDocument60 paginiTropical Infection DiseasesVerarisna100% (1)
- Tropical Infection DiseasesDocument59 paginiTropical Infection DiseasesVerarisnaÎncă nu există evaluări
- Tropical Infection DiseasesDocument59 paginiTropical Infection DiseasesVerarisnaÎncă nu există evaluări
- Tropical Infection DiseasesDocument60 paginiTropical Infection DiseasesVerarisna100% (1)
- Tropical Infection DiseasesDocument60 paginiTropical Infection DiseasesVerarisna100% (1)
- Hepatology: An Introduction to Viral HepatitisDocument50 paginiHepatology: An Introduction to Viral HepatitisDwi WulandariÎncă nu există evaluări
- Tropmed Lecture 4Document78 paginiTropmed Lecture 4VerarisnaÎncă nu există evaluări
- Tropical Infection DiseasesDocument59 paginiTropical Infection DiseasesVerarisnaÎncă nu există evaluări
- Tropmed Lecture 4Document78 paginiTropmed Lecture 4VerarisnaÎncă nu există evaluări
- Disorders of The Wihte CellsDocument22 paginiDisorders of The Wihte CellsVerarisnaÎncă nu există evaluări
- ComaDocument20 paginiComaFebriliana Mao-maoÎncă nu există evaluări
- Tropical Infection DiseasesDocument59 paginiTropical Infection DiseasesVerarisnaÎncă nu există evaluări
- Tropmed Lecture2Document67 paginiTropmed Lecture2VerarisnaÎncă nu există evaluări
- Geriatric Medicine Lecture (Original)Document35 paginiGeriatric Medicine Lecture (Original)VerarisnaÎncă nu există evaluări
- Hepatology: An Introduction to Viral HepatitisDocument50 paginiHepatology: An Introduction to Viral HepatitisDwi WulandariÎncă nu există evaluări
- MgSO4 For EclampsiaDocument10 paginiMgSO4 For EclampsiaVerarisnaÎncă nu există evaluări
- Diah Mustika HW SPS, Kic Intensive Care Unit of Emergency Department Naval Hospital DR RAMELAN, SurabayaDocument15 paginiDiah Mustika HW SPS, Kic Intensive Care Unit of Emergency Department Naval Hospital DR RAMELAN, SurabayaDessy MissaÎncă nu există evaluări
- Tropical Infection DiseasesDocument59 paginiTropical Infection DiseasesVerarisnaÎncă nu există evaluări
- Geriatric Medicine Lecture (Original)Document35 paginiGeriatric Medicine Lecture (Original)VerarisnaÎncă nu există evaluări
- Disorders of The Wihte CellsDocument22 paginiDisorders of The Wihte CellsVerarisnaÎncă nu există evaluări
- Geriatric Medicine Lecture (Original)Document35 paginiGeriatric Medicine Lecture (Original)VerarisnaÎncă nu există evaluări
- Subarachnoid HemorrhageDocument13 paginiSubarachnoid HemorrhageRntiaÎncă nu există evaluări
- Understanding Parkinson's DiseaseDocument65 paginiUnderstanding Parkinson's DiseaseAnonymous awH7zthjgÎncă nu există evaluări
- Test Result Normal Range Interpreta Tion Implicatio NDocument11 paginiTest Result Normal Range Interpreta Tion Implicatio NSitty Aizah MangotaraÎncă nu există evaluări
- Prevalence of Dengue Viral Infections Among Febrile Patients in Mombasa County, KenyaDocument95 paginiPrevalence of Dengue Viral Infections Among Febrile Patients in Mombasa County, KenyaMuhammad AyazÎncă nu există evaluări
- Part A 3 Dengue FeverDocument9 paginiPart A 3 Dengue Feverfernanda1rondelli100% (1)
- Presentation On Dengue FeverDocument31 paginiPresentation On Dengue FeverDrMuhammad Ishfaq HabibÎncă nu există evaluări
- Jurnal Inggris DBDDocument8 paginiJurnal Inggris DBDMochamadAfifAlyÎncă nu există evaluări
- Emerging Infectious Disease CDC 2016Document172 paginiEmerging Infectious Disease CDC 2016Vera IndrawatiÎncă nu există evaluări
- L 01Document82 paginiL 01411014020Încă nu există evaluări
- បទបង្ហាញCPDខេត្តកណ្តាលDocument160 paginiបទបង្ហាញCPDខេត្តកណ្តាលSothea SotakÎncă nu există evaluări
- 2nd MAPEH 3Document2 pagini2nd MAPEH 3Edmar MejiaÎncă nu există evaluări
- HUMASIS Products Brochure - 2020Document32 paginiHUMASIS Products Brochure - 2020Quan NguyenngocÎncă nu există evaluări
- BHW Pocket HandbookDocument70 paginiBHW Pocket HandbookGa B B Orlongan100% (9)
- Concept Map Group 1Document1 paginăConcept Map Group 1eric macabiog100% (1)
- Cong GengueDocument4 paginiCong GengueSiti Hidayatul FitriÎncă nu există evaluări
- Dengue PoathoDocument6 paginiDengue PoathoCleobebs Agustin100% (1)
- 640-663 ImciDocument25 pagini640-663 ImciYaj Cruzada100% (1)
- Csec HSB June 2011 p2Document16 paginiCsec HSB June 2011 p2Sachin Bahadoorsingh100% (1)
- Dengue Fever EngDocument17 paginiDengue Fever EngRia Tustina HendrayaniÎncă nu există evaluări
- Exam Question Bi Form2Document11 paginiExam Question Bi Form2Princess DyanaÎncă nu există evaluări
- Care PlansDocument67 paginiCare PlansShaina Fe RabaneraÎncă nu există evaluări
- Dengue MGMTDocument1 paginăDengue MGMTkumar23Încă nu există evaluări
- Dengue Shock Syndrome: Dr. Elsye Souvriyanti, SpaDocument18 paginiDengue Shock Syndrome: Dr. Elsye Souvriyanti, SpaYesi Maulani NovitasariÎncă nu există evaluări
- Literature ReviewDocument3 paginiLiterature ReviewWaleed AhmedÎncă nu există evaluări
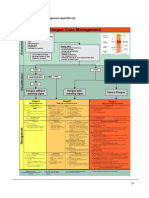
- Management Severe DengueDocument18 paginiManagement Severe DengueMuhammad Fhandeka IsrarÎncă nu există evaluări
- Dengue Disease Spectrum Among Infants in The 2001 Dengue Epidemic in Chennai, Tamil Nadu, IndiaDocument3 paginiDengue Disease Spectrum Among Infants in The 2001 Dengue Epidemic in Chennai, Tamil Nadu, IndiaReju VijayandranÎncă nu există evaluări
- Pictorial Keys For The Identification of MosquitoesDocument60 paginiPictorial Keys For The Identification of MosquitoesElvis Bernal Campos100% (1)
- NSTP AssignmentDocument9 paginiNSTP AssignmentDiana Ruth ElizagaÎncă nu există evaluări
- Analisis Spasial Tingkat Risiko Wilayah Terhadap DBD (Studi Kasus: Kecamatan Manggala, Panakukkang, Dan Mariso Kota Makassar)Document10 paginiAnalisis Spasial Tingkat Risiko Wilayah Terhadap DBD (Studi Kasus: Kecamatan Manggala, Panakukkang, Dan Mariso Kota Makassar)Afif DhiaulhaqÎncă nu există evaluări
- DOST OL Trap in Schools NationwideDocument13 paginiDOST OL Trap in Schools NationwideEdelyn Olivete CaacbayÎncă nu există evaluări
- Catalogue Biosynex 2016 Vus A4Document32 paginiCatalogue Biosynex 2016 Vus A4Nicu IosefÎncă nu există evaluări
- Effect of Vitamin E On Thrombocytopenia in Dengue FeverDocument5 paginiEffect of Vitamin E On Thrombocytopenia in Dengue FeverBernadeth MeilyÎncă nu există evaluări