S-ar putea să vă placă și
- Denture Stomatitis KP UNissula Mei 2016Document53 paginiDenture Stomatitis KP UNissula Mei 2016Aditya ZulfikarÎncă nu există evaluări
- KP Lesi Pre Kanker Kanker Dan Efek Terapi Kanker Rongga MulutDocument58 paginiKP Lesi Pre Kanker Kanker Dan Efek Terapi Kanker Rongga MulutAditya ZulfikarÎncă nu există evaluări
- Pengaruh Terapi CA Pada Rongga MulutDocument24 paginiPengaruh Terapi CA Pada Rongga MulutAditya ZulfikarÎncă nu există evaluări
- Dok Yusuf (Ekstraoral Radiography)Document72 paginiDok Yusuf (Ekstraoral Radiography)Aditya ZulfikarÎncă nu există evaluări
- Relining, Rebasing Blok 19Document18 paginiRelining, Rebasing Blok 19Aditya ZulfikarÎncă nu există evaluări
- Dok Yusuf (Ekstraoral Radiography)Document72 paginiDok Yusuf (Ekstraoral Radiography)Aditya ZulfikarÎncă nu există evaluări
- Dok Rama (Functional Appliance)Document36 paginiDok Rama (Functional Appliance)Aditya ZulfikarÎncă nu există evaluări
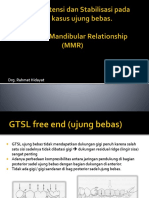
- Dok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRDocument53 paginiDok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRAditya ZulfikarÎncă nu există evaluări
- Periodontal Disease & Systemic, 19 Mei 2017 RevisiDocument25 paginiPeriodontal Disease & Systemic, 19 Mei 2017 RevisiAditya ZulfikarÎncă nu există evaluări
- Komplikasi AlDocument29 paginiKomplikasi AlAditya ZulfikarÎncă nu există evaluări
- Periodontal Disease & Systemic, 19 Mei 2017 RevisiDocument25 paginiPeriodontal Disease & Systemic, 19 Mei 2017 RevisiAditya ZulfikarÎncă nu există evaluări
- Komplikasi AlDocument29 paginiKomplikasi AlAditya ZulfikarÎncă nu există evaluări
- GINGIVAL Disease KulpakDocument61 paginiGINGIVAL Disease KulpakAditya ZulfikarÎncă nu există evaluări
- DRG Ade MSLH Elderely MHSWDocument36 paginiDRG Ade MSLH Elderely MHSWAditya ZulfikarÎncă nu există evaluări
- Dental AnatomyDocument61 paginiDental AnatomyAditya ZulfikarÎncă nu există evaluări
- Dok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRDocument53 paginiDok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRAditya ZulfikarÎncă nu există evaluări
- DRG Ade MSLH Elderely MHSWDocument36 paginiDRG Ade MSLH Elderely MHSWAditya ZulfikarÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Chapter 17 - Oral PathologyDocument50 paginiChapter 17 - Oral PathologyShoyo HinataÎncă nu există evaluări
- Dental Oral Medicine Revision ToolDocument51 paginiDental Oral Medicine Revision ToolAndrew Pritchard75% (4)
- 10.1007@s00405 020 05865 4Document6 pagini10.1007@s00405 020 05865 4noviÎncă nu există evaluări
- Oral Manifestations of Systemic DiseasesDocument14 paginiOral Manifestations of Systemic Diseasesshygal1981Încă nu există evaluări
- CandidiasisDocument1 paginăCandidiasisVpatelÎncă nu există evaluări
- Clinical Aspects of Fungal Infections in DiabetesDocument10 paginiClinical Aspects of Fungal Infections in DiabetesfikriafisÎncă nu există evaluări
- Prevention of Candida Albicans Oral ThrushDocument8 paginiPrevention of Candida Albicans Oral ThrushZkdlin SpaceÎncă nu există evaluări
- Diagnosis and Management of Oral MucositisDocument20 paginiDiagnosis and Management of Oral MucositisAlfyGototronÎncă nu există evaluări
- CH 084 Oral ThrushDocument7 paginiCH 084 Oral ThrushSavir GuptaÎncă nu există evaluări
- 2.acknowledgement and Def Disease CompleteDocument18 pagini2.acknowledgement and Def Disease CompleteStephanie Joy EscalaÎncă nu există evaluări
- T C AnkrahDocument198 paginiT C AnkrahDeep Sleep100% (8)
- Chronic HyperplasticDocument3 paginiChronic HyperplasticrerezÎncă nu există evaluări
- Mycology Board Review Presentation10Document54 paginiMycology Board Review Presentation10Foysal SirazeeÎncă nu există evaluări
- Ilovepdf Merged 1Document193 paginiIlovepdf Merged 1Angelica RatonÎncă nu există evaluări
- PG - Mycology and Prions. 2020Document141 paginiPG - Mycology and Prions. 2020Omeerul RafieÎncă nu există evaluări
- Red Lesions of Oral Cavity A ReviewDocument6 paginiRed Lesions of Oral Cavity A ReviewInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Atlas of Clinical GI Endoscopy 2012 PDFDocument616 paginiAtlas of Clinical GI Endoscopy 2012 PDFKit Chutchit100% (2)
- F. KG - Prosiding - Sri Hernawati - Penatalaksanaan Fisured Tongue Disertai DentureDocument8 paginiF. KG - Prosiding - Sri Hernawati - Penatalaksanaan Fisured Tongue Disertai DentureAlfan MaulanaÎncă nu există evaluări
- Pathogenesis:: Candida Albicans in Gram StainingDocument3 paginiPathogenesis:: Candida Albicans in Gram StainingNida RidzuanÎncă nu există evaluări
- Oral Pathology ModuleDocument31 paginiOral Pathology ModuleDenee Vem MatorresÎncă nu există evaluări
- Fungal InfectionsDocument9 paginiFungal InfectionsCoral Srinivasa RamaluÎncă nu există evaluări
- Oral Candidiasis Causes Types and Treatment PDFDocument12 paginiOral Candidiasis Causes Types and Treatment PDFTiborÎncă nu există evaluări
- Antifungul in DentistryDocument17 paginiAntifungul in DentistryMonaÎncă nu există evaluări
- Oral Manifestations of HIVDocument35 paginiOral Manifestations of HIVfathoni ridwanÎncă nu există evaluări
- Infections of Gastrointestinal TractDocument12 paginiInfections of Gastrointestinal TractEanna ParadoÎncă nu există evaluări
- MycologyDocument117 paginiMycologybanteng wibisonoÎncă nu există evaluări
- Oral Candidiasis Associated With Inhaled Corticosteroid Use: Comparison of Fluticasone and BeclomethasoneDocument6 paginiOral Candidiasis Associated With Inhaled Corticosteroid Use: Comparison of Fluticasone and BeclomethasoneAlia YuddinÎncă nu există evaluări
- Oral Pathology Review List For NDEB With PicsDocument75 paginiOral Pathology Review List For NDEB With PicsBookwyrm AddictÎncă nu există evaluări
- Day 2 Unicorn 1Document279 paginiDay 2 Unicorn 1Gustavo A OrtegonÎncă nu există evaluări
- Neet ENTDocument391 paginiNeet ENTwilliamsjoseff0Încă nu există evaluări