S-ar putea să vă placă și
- Diarrhoea and Vomiting in ChildrenDocument16 paginiDiarrhoea and Vomiting in ChildrenKenny Josef100% (1)
- Diarroea Nice Guidlines PDFDocument16 paginiDiarroea Nice Guidlines PDFFayzaRayesÎncă nu există evaluări
- IMCI UpdatesDocument5 paginiIMCI UpdatesJaypee Ravina100% (2)
- Zinc Advocacy USAIDDocument4 paginiZinc Advocacy USAIDmuamarrayÎncă nu există evaluări
- Gastroenteritis+in+children May2014+Document17 paginiGastroenteritis+in+children May2014+Naily HosenÎncă nu există evaluări
- ARCS Paediatric IV Fluid GuidelinesDocument16 paginiARCS Paediatric IV Fluid GuidelinesWidyadarya Triyono PutriÎncă nu există evaluări
- Fluid Therapy - PICU Oct 2010 PDFDocument4 paginiFluid Therapy - PICU Oct 2010 PDFSiti ChodijahÎncă nu există evaluări
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryDe la EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryÎncă nu există evaluări
- Nutrition Support in Adults NICE Guideline PDFDocument54 paginiNutrition Support in Adults NICE Guideline PDFnewtypeÎncă nu există evaluări
- National Programs Related To Child Health and WelfareDocument61 paginiNational Programs Related To Child Health and WelfareSujata Mishra100% (8)
- Basic Paediatric Protocols - Revised - Sept2010Document47 paginiBasic Paediatric Protocols - Revised - Sept2010Aravind Kumar100% (1)
- Using Insulin Pumps in Diabetes: A Guide for Nurses and Other Health ProfessionalsDe la EverandUsing Insulin Pumps in Diabetes: A Guide for Nurses and Other Health ProfessionalsÎncă nu există evaluări
- Basic Paediatric Protocols 2016Document62 paginiBasic Paediatric Protocols 2016Steven WilliamÎncă nu există evaluări
- NCP Part 1 Overview of NCPDocument23 paginiNCP Part 1 Overview of NCPMa. Ferimi Gleam BajadoÎncă nu există evaluări
- SAM Guidelines IAP Deepak Ugra 10.10.11Document28 paginiSAM Guidelines IAP Deepak Ugra 10.10.11Amit JoshiÎncă nu există evaluări
- Farmako 16-19Document4 paginiFarmako 16-19Rita rukmawatiÎncă nu există evaluări
- Pafp PDF 60 2 163 183Document21 paginiPafp PDF 60 2 163 183Jim TangianÎncă nu există evaluări
- DR Cherise Scott of TB Alliance On What Are The New 1st-Ever Child-Friendly TB DrugsDocument12 paginiDR Cherise Scott of TB Alliance On What Are The New 1st-Ever Child-Friendly TB DrugsbobbyramakantÎncă nu există evaluări
- Acute GastroenteritisDocument38 paginiAcute GastroenteritisMuhammad khairul afizal RohimÎncă nu există evaluări
- Dietary On HDDocument23 paginiDietary On HDKevin OwenÎncă nu există evaluări
- Teneligliptin CommunicationDocument22 paginiTeneligliptin CommunicationBhushan Patil100% (1)
- 3 NationalhealthprogrammesDocument92 pagini3 NationalhealthprogrammesABISHAK RAVIKUMARÎncă nu există evaluări
- Keeping Kids in The Picture: Pediatric TB in The Cops ProcessDocument14 paginiKeeping Kids in The Picture: Pediatric TB in The Cops ProcesskesudeenÎncă nu există evaluări
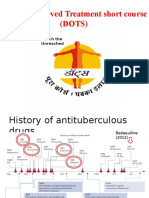
- Dots MD SEMINARDocument48 paginiDots MD SEMINARAlfred MathewÎncă nu există evaluări
- BDA Critical Care Specialist Group COVID-19 Best Practice Guidance: Enteral Feeding in Prone PositionDocument6 paginiBDA Critical Care Specialist Group COVID-19 Best Practice Guidance: Enteral Feeding in Prone PositionMahtosurup GodavarthyÎncă nu există evaluări
- Changes in Pattern of Community Pharmacy Services in The Philippines ForDocument34 paginiChanges in Pattern of Community Pharmacy Services in The Philippines ForJessica EdiosÎncă nu există evaluări
- Parenteral Nutrition InfusionsDocument1 paginăParenteral Nutrition Infusions1stsgtwife4055Încă nu există evaluări
- Doh Programs PDFDocument68 paginiDoh Programs PDFMikaela Lozano100% (1)
- Palliative Care Intervention in The Management of Diabetes - DR Steve JonesDocument30 paginiPalliative Care Intervention in The Management of Diabetes - DR Steve Jonesmalaysianhospicecouncil6240Încă nu există evaluări
- 6.6 Fluid Management Patients With Renal DisordersDocument8 pagini6.6 Fluid Management Patients With Renal Disordersanon_996578489Încă nu există evaluări
- Diarrhoea Guidelines PDFDocument58 paginiDiarrhoea Guidelines PDFmustikaarumÎncă nu există evaluări
- IPHS Guidelines For PHCDocument24 paginiIPHS Guidelines For PHCShwethaÎncă nu există evaluări
- Embedded R D China Interv Trial AMR 29.05.2019 V1aDocument17 paginiEmbedded R D China Interv Trial AMR 29.05.2019 V1aAnonymous gVgLS4Încă nu există evaluări
- Periodontal Management of Medically Compromised Patients (Continued)Document11 paginiPeriodontal Management of Medically Compromised Patients (Continued)Yehya Al KhashabÎncă nu există evaluări
- NCCP, NCDCS, Nutritional PRGMDocument44 paginiNCCP, NCDCS, Nutritional PRGMdarshitkotadiya2553Încă nu există evaluări
- National Health Programme (Part-II) : DR Anil Kumar Agrawal Assisstant ProfessorDocument37 paginiNational Health Programme (Part-II) : DR Anil Kumar Agrawal Assisstant Professoranil agrawalÎncă nu există evaluări
- National Health Programme (Part-II) : DR Anil Kumar Agrawal Assisstant ProfessorDocument37 paginiNational Health Programme (Part-II) : DR Anil Kumar Agrawal Assisstant Professoranil agrawalÎncă nu există evaluări
- Pocket Card Parenteral Nutrition February 2021Document5 paginiPocket Card Parenteral Nutrition February 2021Kouba MarciminiÎncă nu există evaluări
- Total Parenteral Nutrition Guideline-4 - 2Document38 paginiTotal Parenteral Nutrition Guideline-4 - 2Henry M. BarberenaÎncă nu există evaluări
- 7 Nutritional Intervention ClassDocument30 pagini7 Nutritional Intervention ClassWorku KifleÎncă nu există evaluări
- The Hospital Management of Hypoglycaemia in Adults With Diabetes Mellitus 3rd EditionDocument40 paginiThe Hospital Management of Hypoglycaemia in Adults With Diabetes Mellitus 3rd EditionRadoslav FedeevÎncă nu există evaluări
- Class 16, 17 National Health Programmes of NepalDocument61 paginiClass 16, 17 National Health Programmes of NepalRajkishor YadavÎncă nu există evaluări
- Final Nutrition Policies MELLPI Pro PDFDocument99 paginiFinal Nutrition Policies MELLPI Pro PDFboo goo100% (2)
- Pokharel - Intensification of Iron/Folic Acid Supplementation Program in NepalDocument30 paginiPokharel - Intensification of Iron/Folic Acid Supplementation Program in NepalDhaka2012Încă nu există evaluări
- Doctors & DietDocument19 paginiDoctors & Dietrufus_400143616Încă nu există evaluări
- Standard Treatment Protocols in Primary Health Care: Transforming Comprehensive Healthcare in IndiaDocument15 paginiStandard Treatment Protocols in Primary Health Care: Transforming Comprehensive Healthcare in Indiavaishali TMU studentÎncă nu există evaluări
- Moderator: Dr. Arulkumaran Presentor: Dr. NiharikaDocument37 paginiModerator: Dr. Arulkumaran Presentor: Dr. NiharikaMerriyet MbÎncă nu există evaluări
- Basic Paed Protocols January 2016 FinalDocument62 paginiBasic Paed Protocols January 2016 FinalRoberto MainaÎncă nu există evaluări
- Bowel Assessment and Management (Adults, Adolescents, Children, Infants and Neonates)Document31 paginiBowel Assessment and Management (Adults, Adolescents, Children, Infants and Neonates)Sitha ChristineÎncă nu există evaluări
- Archives of Practical Pediatrics 12Document5 paginiArchives of Practical Pediatrics 12Ashok jainÎncă nu există evaluări
- 3.management of DiabetesDocument71 pagini3.management of DiabetesNixon KeyaÎncă nu există evaluări
- Total Parenteral Nutrition Guideline-4 - 2Document38 paginiTotal Parenteral Nutrition Guideline-4 - 2FirnandaÎncă nu există evaluări
- The Hospital Management of Hypoglycaemia in Adults With Diabetes Mellitus 3rd EditionDocument40 paginiThe Hospital Management of Hypoglycaemia in Adults With Diabetes Mellitus 3rd EditionRumahSehat N-CareÎncă nu există evaluări
- Guidelines For Acute Malnutrition (Somalia)Document132 paginiGuidelines For Acute Malnutrition (Somalia)Muhammad Fitrah Noor67% (6)
- Clinical Guideline 10: Type 2 DiabetesDocument2 paginiClinical Guideline 10: Type 2 Diabetesalvin0033Încă nu există evaluări
- Diabetes for Primary Care: A Step By Step ApproachDe la EverandDiabetes for Primary Care: A Step By Step ApproachÎncă nu există evaluări
- Kidney Disease Management: A Practical Approach for the Non-Specialist Healthcare PractitionerDe la EverandKidney Disease Management: A Practical Approach for the Non-Specialist Healthcare PractitionerÎncă nu există evaluări
- Fix Your Genes to Fit Your Jeans: Optimizing Diet, Health and Weight Through Personal GeneticsDe la EverandFix Your Genes to Fit Your Jeans: Optimizing Diet, Health and Weight Through Personal GeneticsÎncă nu există evaluări
- Kidney TransplantDocument3 paginiKidney TransplantSuneel Kumar PrajapatiÎncă nu există evaluări
- Sharon Denise Gross: 513 Grazing Field Drive, Tuscaloosa, AL 35405 (C) 205-242-3670 (W) 205-554-2000 Ext. 3617 (E) (E)Document6 paginiSharon Denise Gross: 513 Grazing Field Drive, Tuscaloosa, AL 35405 (C) 205-242-3670 (W) 205-554-2000 Ext. 3617 (E) (E)api-469030612Încă nu există evaluări
- Nclex PointersDocument4 paginiNclex PointersCarl Michael de Guzman75% (12)
- Role of Pain Placebo Analgesia: Gordont, Fields FDocument4 paginiRole of Pain Placebo Analgesia: Gordont, Fields Fmaurina rizkiÎncă nu există evaluări
- Buku OrthopaediDocument6 paginiBuku OrthopaediPriza RazunipÎncă nu există evaluări
- Bacterial Sinusitis in Children: AcuteDocument11 paginiBacterial Sinusitis in Children: AcutefriscahalimÎncă nu există evaluări
- DAFTAR PUSTAKA (Kasus Mendalam 2)Document4 paginiDAFTAR PUSTAKA (Kasus Mendalam 2)mkpnurdinÎncă nu există evaluări
- Idiopathic Hypersomnia Its All in Their HeadDocument2 paginiIdiopathic Hypersomnia Its All in Their HeadSambo Pembasmi LemakÎncă nu există evaluări
- DT311 TPS Bahasa Inggris - Ani - CBT - Paket 1Document4 paginiDT311 TPS Bahasa Inggris - Ani - CBT - Paket 1Eki BBÎncă nu există evaluări
- Screenshot 2021-06-23 at 11.36.48 AMDocument116 paginiScreenshot 2021-06-23 at 11.36.48 AMSmitha ShekarÎncă nu există evaluări
- Pharm 451-Historical Development of Chemotherapy 2021Document22 paginiPharm 451-Historical Development of Chemotherapy 2021Akowuah SamuelÎncă nu există evaluări
- Urinary Tract InfectionsDocument44 paginiUrinary Tract Infectionstummalapalli venkateswara rao100% (2)
- Bllod Transfision ConsentDocument1 paginăBllod Transfision ConsentumeshbhartiÎncă nu există evaluări
- Bhs InggrisDocument4 paginiBhs InggrisNUR WULAN SARIÎncă nu există evaluări
- Benign Tumours of LarynxDocument35 paginiBenign Tumours of LarynxMidhun Thomas EdathinalÎncă nu există evaluări
- EPN Book 2Document40 paginiEPN Book 2Budhi Priyanto DitaraÎncă nu există evaluări
- The Study of Drug Resistance in Bacteria Using Antibiotics: June 2019Document6 paginiThe Study of Drug Resistance in Bacteria Using Antibiotics: June 20197'A'06Aditya BeheraÎncă nu există evaluări
- Things To Read: A. Trauma: Fractures and DislocationsDocument4 paginiThings To Read: A. Trauma: Fractures and DislocationsHanien YeeÎncă nu există evaluări
- 04 Tetanus BDocument12 pagini04 Tetanus BRahmatul YasiroÎncă nu există evaluări
- Superior PDFDocument5 paginiSuperior PDFmhgc108210Încă nu există evaluări
- Scullard Shock and Infection PDFDocument53 paginiScullard Shock and Infection PDFDave WilliamzÎncă nu există evaluări
- Outbreak Investigation Case Scenarios-PHASE III-SDL, 15-17.05.2023-1Document13 paginiOutbreak Investigation Case Scenarios-PHASE III-SDL, 15-17.05.2023-1srinidhi premkumarÎncă nu există evaluări
- Activity 3.1.2 Rapid Pathogen IdentificationDocument8 paginiActivity 3.1.2 Rapid Pathogen Identificationsahsdjkh7Încă nu există evaluări
- Is Critical To Your Health How The Parasympathetic StateDocument56 paginiIs Critical To Your Health How The Parasympathetic Stateigor petrovskiÎncă nu există evaluări
- Anti Tuberculosis AgentsDocument15 paginiAnti Tuberculosis Agentsejg26100% (1)
- Ob2 Sas 40Document7 paginiOb2 Sas 40????Încă nu există evaluări
- Case Study BipolarDocument12 paginiCase Study Bipolarapi-353954238Încă nu există evaluări
- Can Trees Get CancerDocument2 paginiCan Trees Get CancerSimarpreet Kaur 1025Încă nu există evaluări
- Baichongwo (M-Le-34) : Hundred Insect BurrowDocument1 paginăBaichongwo (M-Le-34) : Hundred Insect Burrowray72roÎncă nu există evaluări
- Bragdon V AbbottDocument22 paginiBragdon V AbbottZÎncă nu există evaluări