S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Foot reflexology chart shows how hand acupressure points relate to body partsDocument3 paginiFoot reflexology chart shows how hand acupressure points relate to body partsgautamlipika100% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Advances in Extraction TechniquesDocument13 paginiAdvances in Extraction TechniquesashajangamÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- IV Therapy SsDocument56 paginiIV Therapy Sssaeed_chohan100% (8)
- Eric Berg CVDocument6 paginiEric Berg CVHaralambicÎncă nu există evaluări
- Hangnails and HomoeopathyDocument7 paginiHangnails and HomoeopathyDr. Rajneesh Kumar Sharma MD HomÎncă nu există evaluări
- Understanding-Ocd 2016 v2Document27 paginiUnderstanding-Ocd 2016 v2Samanjit Sen Gupta100% (1)
- DRUG STUDY PsycheDocument1 paginăDRUG STUDY Psychejulesubayubay5428100% (1)
- Advanced Burn Life SupportDocument118 paginiAdvanced Burn Life SupportIntan Noa100% (1)
- Blood Bank ChecklistDocument4 paginiBlood Bank ChecklistFIAZ MAQBOOL FAZILIÎncă nu există evaluări
- July 2017 SepsisDocument73 paginiJuly 2017 SepsislilyrbrtÎncă nu există evaluări
- I NewDocument4 paginiI NewlilyrbrtÎncă nu există evaluări
- UrticariaDocument12 paginiUrticarialilyrbrtÎncă nu există evaluări
- 2015 PMR Guidelines PDFDocument12 pagini2015 PMR Guidelines PDFlilyrbrtÎncă nu există evaluări
- Int Obs PDFDocument37 paginiInt Obs PDFsurgeon77Încă nu există evaluări
- Theory and Practice of Pure Tone Audiometry - PTADocument12 paginiTheory and Practice of Pure Tone Audiometry - PTAsolhazÎncă nu există evaluări
- The Use of Superficial Heat For Treatment of TempoDocument6 paginiThe Use of Superficial Heat For Treatment of TempoJulianaÎncă nu există evaluări
- US Elsevier Health Bookshop - Mosby, Saunders, Netter & MoreDocument4 paginiUS Elsevier Health Bookshop - Mosby, Saunders, Netter & MoreWilmer Zambrano GuerreroÎncă nu există evaluări
- Chapter 15 - Hormones & Endocrine GlandsDocument17 paginiChapter 15 - Hormones & Endocrine Glandsapi-3728508100% (1)
- Comparison of The Thesslay Test and McMurray Test - A Systematic Review of Comparative Diagnostic StudiesDocument7 paginiComparison of The Thesslay Test and McMurray Test - A Systematic Review of Comparative Diagnostic StudiesCambriaChicoÎncă nu există evaluări
- Shaw 2004Document7 paginiShaw 2004Mouloudi NajouaÎncă nu există evaluări
- Introduction To Nursing PharmacologyDocument5 paginiIntroduction To Nursing PharmacologyJon Adam Bermudez SamatraÎncă nu există evaluări
- Bull InfertilDocument29 paginiBull InfertilYonaaasÎncă nu există evaluări
- Cervical Lymphoepithelial CystDocument6 paginiCervical Lymphoepithelial CystAhmed Al-jumailiÎncă nu există evaluări
- Hypokalemia and Hyperkalemia in Infants and Children: Pathophysiology and TreatmentDocument11 paginiHypokalemia and Hyperkalemia in Infants and Children: Pathophysiology and TreatmentAnantaBenvenutoÎncă nu există evaluări
- Optima GutDocument11 paginiOptima GutNoly ClaveringÎncă nu există evaluări
- Expression of MDM2 and p16 in AngiomyolipomaDocument7 paginiExpression of MDM2 and p16 in AngiomyolipomaTiago TavaresÎncă nu există evaluări
- COVID-19 Patient Report SummaryDocument2 paginiCOVID-19 Patient Report Summarymuhammad imranÎncă nu există evaluări
- Week 29 - DRRRDocument5 paginiWeek 29 - DRRRMira VeranoÎncă nu există evaluări
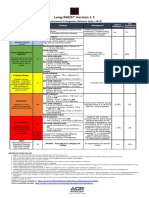
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Document1 paginăLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotÎncă nu există evaluări
- Anterior Cruciate Ligament InjuryDocument3 paginiAnterior Cruciate Ligament InjuryAdrian Nazario PragachaÎncă nu există evaluări
- ImmunosuppresentsDocument13 paginiImmunosuppresentsmadeputraÎncă nu există evaluări
- Prevalence of Hypothyroidism in Adults An EpidemioDocument6 paginiPrevalence of Hypothyroidism in Adults An EpidemioCindy Auliah NasutionÎncă nu există evaluări
- Abu Dhabi DRGDocument62 paginiAbu Dhabi DRGDolly creationsÎncă nu există evaluări
- FormsDocument15 paginiFormsBiswajit DasÎncă nu există evaluări