S-ar putea să vă placă și
- Derma NotesDocument52 paginiDerma NotesUsmanÎncă nu există evaluări
- Skin-PathologyDocument32 paginiSkin-PathologyArfa BaigÎncă nu există evaluări
- 1.introduction To DermatologyDocument57 pagini1.introduction To DermatologyMutasım Battah100% (2)
- Skin Conditions Part II-1Document54 paginiSkin Conditions Part II-1mohamedkallon1996Încă nu există evaluări
- Skin Conditions 1) Eczema & Dermatitis 2) Acne 3) Athletes Foot 4) Warts & Verrucae 5) Scabies Scabies Mite "Sarcoptes Scabiei"Document4 paginiSkin Conditions 1) Eczema & Dermatitis 2) Acne 3) Athletes Foot 4) Warts & Verrucae 5) Scabies Scabies Mite "Sarcoptes Scabiei"2288RÎncă nu există evaluări
- Q.1 Components of Skin: The Skin: Basic Structure and FunctionDocument7 paginiQ.1 Components of Skin: The Skin: Basic Structure and Functionnani100Încă nu există evaluări
- LCD Efloresensi Dr. PS 2017Document85 paginiLCD Efloresensi Dr. PS 2017Hemeshwary KumaraveluÎncă nu există evaluări
- Skin LesionsDocument14 paginiSkin Lesionsbhat junaidÎncă nu există evaluări
- Basic Skin Lesions PDFDocument121 paginiBasic Skin Lesions PDFimdad khanÎncă nu există evaluări
- Module 1 LabDocument75 paginiModule 1 Labkrystal ongÎncă nu există evaluări
- Morfologi Kelainan KulitDocument67 paginiMorfologi Kelainan KulitLovina Falendini AndriÎncă nu există evaluări
- Microbial Diseases of The Skin-1Document84 paginiMicrobial Diseases of The Skin-1wllmaanka4Încă nu există evaluări
- Skin, Hair, and Nails AssessmentDocument44 paginiSkin, Hair, and Nails Assessmentعمر حليم omar haleem100% (1)
- Diseases of SkinDocument18 paginiDiseases of SkinrishikeshkallaÎncă nu există evaluări
- Integument System PATH-321Document29 paginiIntegument System PATH-321abdullahÎncă nu există evaluări
- Skinhairnail Ass 1Document43 paginiSkinhairnail Ass 1Airene Aquino BusaniaÎncă nu există evaluări
- Skin Examination: Dr. Ploesteanu Rodica Emergency Hospital Sfantul Pantelimon" 2018Document167 paginiSkin Examination: Dr. Ploesteanu Rodica Emergency Hospital Sfantul Pantelimon" 2018Arleen MatincaÎncă nu există evaluări
- UNIT - IV Assesment of Skin Head and NeckDocument48 paginiUNIT - IV Assesment of Skin Head and Neckraima ayazÎncă nu există evaluări
- Psoriasis BBBDocument28 paginiPsoriasis BBBPramod ChoudharyÎncă nu există evaluări
- IntegumentaryDocument54 paginiIntegumentaryA-Mark Gabriel PesanteÎncă nu există evaluări
- Commonskindiseases 150110033432 Conversion Gate02 1Document70 paginiCommonskindiseases 150110033432 Conversion Gate02 1Dr. Siraphop OneSongchai RatanasubanÎncă nu există evaluări
- Prev Next: © 2014 Webmd, Llc. All Rights ReservedDocument5 paginiPrev Next: © 2014 Webmd, Llc. All Rights ReservedOlfaktorius GoenawanÎncă nu există evaluări
- Skin AssessmentDocument45 paginiSkin AssessmentAbdurehman AyeleÎncă nu există evaluări
- Dermatosis-WPS Office-1Document111 paginiDermatosis-WPS Office-1PriyaÎncă nu există evaluări
- Disorders of Sebaceous GlandDocument54 paginiDisorders of Sebaceous GlandAnurag PandeyÎncă nu există evaluări
- 1) Bacterial Skin InfDocument32 pagini1) Bacterial Skin InfsmrutuÎncă nu există evaluări
- Paediatric Dermatology (Notes)Document24 paginiPaediatric Dermatology (Notes)Ahmad Syarafi AbdullahÎncă nu există evaluări
- Benign Gynecologic LesionsDocument53 paginiBenign Gynecologic LesionsChristopher Goodman-SmithÎncă nu există evaluări
- Acne VulgarisDocument60 paginiAcne Vulgarischarmaine_olivia_1100% (2)
- 008 Skin Hair NailsDocument35 pagini008 Skin Hair NailsPauline An Toni CapurihanÎncă nu există evaluări
- Year 5 PSE Session 2 OSCE Practice May 2014Document170 paginiYear 5 PSE Session 2 OSCE Practice May 2014Mohd KhalilÎncă nu există evaluări
- ImpetigoDocument5 paginiImpetigoInges PSÎncă nu există evaluări
- Skins - : Starting OffDocument25 paginiSkins - : Starting OffSilviuÎncă nu există evaluări
- Skin LesionsDocument4 paginiSkin LesionsRose Marceline Patague TalubanÎncă nu există evaluări
- Zoe Yichang Central People's HospitalDocument32 paginiZoe Yichang Central People's HospitalMohsin Tanmoy100% (1)
- PENDAHULUAN - EfloresensiDocument50 paginiPENDAHULUAN - EfloresensiSucitri NyomanÎncă nu există evaluări
- Disorders and Diseases of The SkinDocument109 paginiDisorders and Diseases of The Skindaniellestrok8947100% (1)
- Types of Primary Skin LesionsDocument4 paginiTypes of Primary Skin LesionsKat TaasinÎncă nu există evaluări
- Dr. R. Sekhon - Dermatology Telehealth Jan 27 MRDocument45 paginiDr. R. Sekhon - Dermatology Telehealth Jan 27 MRAnissa ADÎncă nu există evaluări
- PsoriasisDocument23 paginiPsoriasisvasavavipul38022Încă nu există evaluări
- Kuliah Sindrom Rabu 19112008.Document65 paginiKuliah Sindrom Rabu 19112008.Nurdiana RahmadaniÎncă nu există evaluări
- L1,2,3 - Intro, Anatomy, Language of Dermatologydr. Almontaser BellahDocument102 paginiL1,2,3 - Intro, Anatomy, Language of Dermatologydr. Almontaser BellahTOMMYÎncă nu există evaluări
- Terminology in DermatologyDocument8 paginiTerminology in DermatologyHesbon MomanyiÎncă nu există evaluări
- Complete Medical Guide for Disease Volume VII; Atopic DermatitisDe la EverandComplete Medical Guide for Disease Volume VII; Atopic DermatitisÎncă nu există evaluări
- Module 3 HomeworkDocument6 paginiModule 3 HomeworkCj LinceÎncă nu există evaluări
- Clinical Overview of Acne Vulgaris: Rich Callahan MSPA, PA-C ICM I - Summer 2009Document22 paginiClinical Overview of Acne Vulgaris: Rich Callahan MSPA, PA-C ICM I - Summer 2009Christopher DennisÎncă nu există evaluări
- Skin An Essential Organ-IIDocument30 paginiSkin An Essential Organ-IIsameen tahirÎncă nu există evaluări
- Dermatology Class NotesDocument48 paginiDermatology Class Notesapi-26938624100% (6)
- Eczematous Disorders CFM REPORT 2Document32 paginiEczematous Disorders CFM REPORT 2Arianne CortezÎncă nu există evaluări
- Skin DisordersDocument202 paginiSkin DisordersMj Briones100% (1)
- Primary and Secondary Skin Lesions - IJDocument43 paginiPrimary and Secondary Skin Lesions - IJThanh Thảo Huỳnh ThịÎncă nu există evaluări
- 08-Skin TumoursDocument8 pagini08-Skin TumoursChris Tan100% (1)
- Bacterial - Viral InfectionsDocument61 paginiBacterial - Viral InfectionsMoayad NawaflehÎncă nu există evaluări
- Cos - Chapter 8 Skin DisordersDocument7 paginiCos - Chapter 8 Skin DisorderssofiaÎncă nu există evaluări
- Cos - Chapter 8 Skin DisordersDocument7 paginiCos - Chapter 8 Skin DisordersALIÎncă nu există evaluări
- Dermatology NotesDocument37 paginiDermatology NotesTamilmani n.mÎncă nu există evaluări
- SkinDocument167 paginiSkinMurti GutoÎncă nu există evaluări
- Acne Vulgaris L2Document33 paginiAcne Vulgaris L2Roshandiep GillÎncă nu există evaluări
- DermaDocument30 paginiDermalydia_chandraÎncă nu există evaluări
- Exfoliative Dermatitis, (Erythroderma) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandExfoliative Dermatitis, (Erythroderma) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- The Cell Biology of Rabies Virus: Using Stealth To Reach The BrainDocument11 paginiThe Cell Biology of Rabies Virus: Using Stealth To Reach The BrainFlavius AnghelÎncă nu există evaluări
- Reviews: Influenza: Lessons From Past Pandemics, Warnings From Current IncidentsDocument10 paginiReviews: Influenza: Lessons From Past Pandemics, Warnings From Current IncidentsFlavius AnghelÎncă nu există evaluări
- Reviews: Influenza: Lessons From Past Pandemics, Warnings From Current IncidentsDocument10 paginiReviews: Influenza: Lessons From Past Pandemics, Warnings From Current IncidentsFlavius AnghelÎncă nu există evaluări
- MicozeDocument68 paginiMicozeFlavius Anghel100% (1)
- Perspective: Allergic Host DefencesDocument8 paginiPerspective: Allergic Host DefencesFlavius AnghelÎncă nu există evaluări
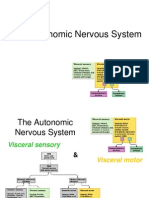
- Lecture 15 - Autonomic Nervous SystemDocument26 paginiLecture 15 - Autonomic Nervous SystemFlavius AnghelÎncă nu există evaluări
- Mechanical Ventilation and Intracranial PressureDocument30 paginiMechanical Ventilation and Intracranial PressureFlavius AnghelÎncă nu există evaluări
- Contraceptive Physiology: by Dr.M.Anthony David MD Professor of PhysiologyDocument44 paginiContraceptive Physiology: by Dr.M.Anthony David MD Professor of PhysiologyFlavius AnghelÎncă nu există evaluări
- Fixed Drug Eruption, Bolognia DermatologyDocument2 paginiFixed Drug Eruption, Bolognia Dermatologyjacob89Încă nu există evaluări
- Pediatric DermatologyDocument47 paginiPediatric DermatologyAmr Abualrub100% (2)
- Varicella and Herpes ZosterDocument20 paginiVaricella and Herpes ZosterzakiÎncă nu există evaluări
- PemphigusDocument1 paginăPemphigusiSmayli (smyle-smayl)Încă nu există evaluări
- Skin DisordersDocument202 paginiSkin DisordersMj Briones100% (1)
- Neonatal Diseases PDFDocument41 paginiNeonatal Diseases PDFmomobelle100% (1)
- Papulosquamous Ds.Document70 paginiPapulosquamous Ds.CHALIE MEQUÎncă nu există evaluări
- Icd10 CM Quick CoderDocument2 paginiIcd10 CM Quick CoderErez Tryaza Himura50% (2)
- LedesmaDocument6 paginiLedesmaAngela Dimaano SaladaÎncă nu există evaluări
- Tine ADocument6 paginiTine AMemo AliÎncă nu există evaluări
- Dermatology Made EasyDocument46 paginiDermatology Made EasyHeather Marie Mathis100% (1)
- Fever and RashDocument33 paginiFever and RashVarun B RenukappaÎncă nu există evaluări
- Hyperpigmented DisorderDocument49 paginiHyperpigmented Disorderضبيان فرحانÎncă nu există evaluări
- HerpesDocument2 paginiHerpesSyafruddin GBÎncă nu există evaluări
- Revision Oral Pathology: Dr. Nermine El BaheyDocument58 paginiRevision Oral Pathology: Dr. Nermine El BaheyEslam abokhalilÎncă nu există evaluări
- Om Fix 2019Document281 paginiOm Fix 2019Sinta Gayatri100% (1)
- Part I Travel Documents Issued by Third Countries and Territorial Entities en 0Document124 paginiPart I Travel Documents Issued by Third Countries and Territorial Entities en 0drlazyboyÎncă nu există evaluări
- Pityriasis AlbaDocument6 paginiPityriasis AlbaLee Eng SiangÎncă nu există evaluări
- Trichofolliculome PDFDocument3 paginiTrichofolliculome PDFSak SltÎncă nu există evaluări
- Pen FigoDocument2 paginiPen FigoCaro SepulvedaÎncă nu există evaluări
- Cos - Chapter 8 Skin DisordersDocument7 paginiCos - Chapter 8 Skin DisordersALIÎncă nu există evaluări
- Errichetti2019 - Patrones en DermatosDocument14 paginiErrichetti2019 - Patrones en DermatosLaura GarciaÎncă nu există evaluări
- Scabies Home Remedies Treatment and ImagesDocument3 paginiScabies Home Remedies Treatment and ImagesIyan DwiÎncă nu există evaluări
- Dermatitis DR Citra 260907Document56 paginiDermatitis DR Citra 260907Adam AriwibawaÎncă nu există evaluări
- Skin and Body Membranes For AnaPhyDocument3 paginiSkin and Body Membranes For AnaPhyJASHEL M. CASTANARESÎncă nu există evaluări
- Common Skin Problem During AdolescenceDocument12 paginiCommon Skin Problem During AdolescenceKristela Mae ColomaÎncă nu există evaluări
- Great Atlas of Dermatology IndexedDocument73 paginiGreat Atlas of Dermatology Indexedjohn pauloÎncă nu există evaluări
- Dermoscopy of Inflamed Seborrheic KeratosisDocument9 paginiDermoscopy of Inflamed Seborrheic KeratosisFreddy RojasÎncă nu există evaluări
- Kesh Dant NakhDocument6 paginiKesh Dant Nakhdouble slit photon50% (2)
- Seborrheic DermatitisDocument4 paginiSeborrheic DermatitisMuti IlmarifaÎncă nu există evaluări