S-ar putea să vă placă și
- Hidden History of Money & New World Order Usury-730Document730 paginiHidden History of Money & New World Order Usury-730Keith Knight100% (12)
- Diseases of The Vagina, Vulva and Cervix Diseases of The Vagina, Vulva and CervixDocument96 paginiDiseases of The Vagina, Vulva and Cervix Diseases of The Vagina, Vulva and CervixMukesh Thakur100% (1)
- Vaginal DischargeDocument47 paginiVaginal DischargeGladstone AsadÎncă nu există evaluări
- Pelvic Inflammatory DiseaseDocument47 paginiPelvic Inflammatory DiseaseNur Aliya IshakÎncă nu există evaluări
- Pelvic InfectionsDocument56 paginiPelvic Infectionsvein94Încă nu există evaluări
- Infection in Pregnancy PDFDocument39 paginiInfection in Pregnancy PDFsimmyvashisht100% (1)
- Color Theory AdvancedDocument51 paginiColor Theory AdvancedHervis FantiniÎncă nu există evaluări
- A Simple Guide to Sexually Transmitted DiseasesDe la EverandA Simple Guide to Sexually Transmitted DiseasesEvaluare: 5 din 5 stele5/5 (9)
- Lane J 1953 - Neotropical Culicidae Vol IDocument550 paginiLane J 1953 - Neotropical Culicidae Vol IDavid Schiemann100% (3)
- Vulvovaginitis: by James Holencik, DODocument70 paginiVulvovaginitis: by James Holencik, DOSyarifa YuliaÎncă nu există evaluări
- Sexuality PowerpointDocument15 paginiSexuality PowerpointHervis FantiniÎncă nu există evaluări
- GNM TestimonialsDocument110 paginiGNM Testimonialswwildwind50% (2)
- Pelvic Inflammatory Disease and Vaginal DischargeDocument50 paginiPelvic Inflammatory Disease and Vaginal DischargeAbdulrahman NajiÎncă nu există evaluări
- Sexually Transmitted Diseases : (Gonorrhea, Syphilis & Aids)Document54 paginiSexually Transmitted Diseases : (Gonorrhea, Syphilis & Aids)joel david knda mjÎncă nu există evaluări
- LIVERDISEASEDocument82 paginiLIVERDISEASEHervis FantiniÎncă nu există evaluări
- Vector ControlDocument11 paginiVector ControlMayuri Vohra100% (1)
- Pelvic Inflammatory DiseaseDocument17 paginiPelvic Inflammatory DiseaseGhaliey AzizÎncă nu există evaluări
- Vaginitis and PID: Wanda Ronner, M.DDocument17 paginiVaginitis and PID: Wanda Ronner, M.DMunkhjargal BatmunkhÎncă nu există evaluări
- Vaginitis and PID: Wanda Ronner, M.DDocument17 paginiVaginitis and PID: Wanda Ronner, M.DherryÎncă nu există evaluări
- Vaginitis and PID: Wanda Ronner, M.DDocument16 paginiVaginitis and PID: Wanda Ronner, M.DFauzul Nurul AzmiÎncă nu există evaluări
- Dr. Taubel's STD Lecture, Part 2Document67 paginiDr. Taubel's STD Lecture, Part 2f3er3Încă nu există evaluări
- Common STI's in General PracticeDocument52 paginiCommon STI's in General Practice201802027 Mayada ArmaatusÎncă nu există evaluări
- WCLF E1 J 66 F YPUTf 0149Document165 paginiWCLF E1 J 66 F YPUTf 0149ClintonÎncă nu există evaluări
- (Pelvic Inflammatory Disease) Samiya AhmedDocument31 pagini(Pelvic Inflammatory Disease) Samiya AhmedSaamiya AhmedÎncă nu există evaluări
- PID PresentationDocument23 paginiPID Presentationakankiza.lucky83Încă nu există evaluări
- 2 PidDocument31 pagini2 PidNatif BoteÎncă nu există evaluări
- Pelvic Inflammatory Disease: DR TitiDocument68 paginiPelvic Inflammatory Disease: DR TitiSiti NurhasanahÎncă nu există evaluări
- Pid by Chandan KumarDocument68 paginiPid by Chandan KumarChandan Kumar KaushikÎncă nu există evaluări
- Case Discussion: Common Reproductive Tract Infections in WomenDocument63 paginiCase Discussion: Common Reproductive Tract Infections in WomenIea Del PradoÎncă nu există evaluări
- 1 PidDocument44 pagini1 PiddeepaÎncă nu există evaluări
- Intrauterine InfectionDocument17 paginiIntrauterine InfectionAndhika Aryandhie DwiputraÎncă nu există evaluări
- Infections of Female Genital TractDocument67 paginiInfections of Female Genital TractSana AftabÎncă nu există evaluări
- 54.vaginal DischargeDocument40 pagini54.vaginal DischargebenÎncă nu există evaluări
- Dr. Abdel-Fattah Salem M.B.B.CH., D.G.O., M.R.C.O.G., F.R.C.O.GDocument87 paginiDr. Abdel-Fattah Salem M.B.B.CH., D.G.O., M.R.C.O.G., F.R.C.O.Gamneh123Încă nu există evaluări
- Pelvic Inflammatory DiseaseDocument25 paginiPelvic Inflammatory DiseasedeepaÎncă nu există evaluări
- Vulvovaginal InfectionDocument66 paginiVulvovaginal InfectionRadhika BambhaniaÎncă nu există evaluări
- PID LectureDocument41 paginiPID LectureHarold Gabriel Sanchez DelgadoÎncă nu există evaluări
- 5.b.intrauterine InfectionDocument31 pagini5.b.intrauterine InfectionPriyanka Dyah SetioriniÎncă nu există evaluări
- Week 7 - Cystitis&Vaginal ThrushDocument17 paginiWeek 7 - Cystitis&Vaginal Thrushenglishspeak95Încă nu există evaluări
- 51 Vaginal Discharge & PIDDocument45 pagini51 Vaginal Discharge & PIDcollinsmagÎncă nu există evaluări
- Salpingitis and Related DiseasesDocument20 paginiSalpingitis and Related DiseasesSupekshya ShresthaÎncă nu există evaluări
- Vaginal Discharge and Vulvar Disease FinalDocument61 paginiVaginal Discharge and Vulvar Disease FinalrohitÎncă nu există evaluări
- Vaginitis and Vaginal DischargeDocument52 paginiVaginitis and Vaginal Dischargedrdoaabakhet148Încă nu există evaluări
- Presentation Abnormal PuerperiumDocument52 paginiPresentation Abnormal PuerperiumTesfaye AbebeÎncă nu există evaluări
- Medical Microbiology: Sti (STD)Document90 paginiMedical Microbiology: Sti (STD)Brother GeorgeÎncă nu există evaluări
- Pelvic Inflammatory Disease (PID) : Infeksi Menular Seksual (Ims)Document21 paginiPelvic Inflammatory Disease (PID) : Infeksi Menular Seksual (Ims)radianiÎncă nu există evaluări
- Pelvic Inflammatory Disease: A Condition Requiring Closer AttentionDocument44 paginiPelvic Inflammatory Disease: A Condition Requiring Closer AttentionMuhammad Shayan FarooqÎncă nu există evaluări
- Pelvic Inflammatory DiseaseDocument41 paginiPelvic Inflammatory DiseaseEvellyna MeilanyÎncă nu există evaluări
- (Sexually Transmitted Infections) : By. Mrs. MurtiningsihDocument21 pagini(Sexually Transmitted Infections) : By. Mrs. MurtiningsihraiÎncă nu există evaluări
- CD6 2021 STDDocument96 paginiCD6 2021 STDNhelia Santos BañagaÎncă nu există evaluări
- Sexually Transmitted Diseases: Nelia B. Perez RN, MSN Class 2015Document94 paginiSexually Transmitted Diseases: Nelia B. Perez RN, MSN Class 2015Mariana CreciunÎncă nu există evaluări
- Repro Female Repro DisordersDocument11 paginiRepro Female Repro Disordersloli popÎncă nu există evaluări
- Nagati DaflonDocument45 paginiNagati DaflonMohamed Atef MohamedÎncă nu există evaluări
- STIs O & GDocument59 paginiSTIs O & GNoraÎncă nu există evaluări
- Abdominal Pain in Gynecology Non PregnantDocument34 paginiAbdominal Pain in Gynecology Non PregnantRyantino IrdanÎncă nu există evaluări
- Visual Inspection With Acetic Acid (Via)Document38 paginiVisual Inspection With Acetic Acid (Via)Princess Jeanne Roque GairanodÎncă nu există evaluări
- Pelvic Inflammatory DiseaseDocument9 paginiPelvic Inflammatory DiseaseanweshaÎncă nu există evaluări
- Gyne - (Section B) PID-STI-1Document45 paginiGyne - (Section B) PID-STI-1Kailash KhatriÎncă nu există evaluări
- Acute Gynaecological EmergenciesDocument22 paginiAcute Gynaecological EmergenciesMuhammad AmeenÎncă nu există evaluări
- Sexually Transmitted DiseaseDocument36 paginiSexually Transmitted DiseasesmrutuÎncă nu există evaluări
- Reproductive Tract InfectionsDocument46 paginiReproductive Tract Infectionskb100% (1)
- Genital Infections: Assoc Prof Suna KABİL KUCURDocument41 paginiGenital Infections: Assoc Prof Suna KABİL KUCURasdÎncă nu există evaluări
- GYN 讀書報告Document67 paginiGYN 讀書報告Chia-Yuan ChenÎncă nu există evaluări
- Gonorrhea LectureDocument36 paginiGonorrhea LectureMalar VizhiÎncă nu există evaluări
- InfertilityDocument23 paginiInfertilityanduamlakmolalgn332Încă nu există evaluări
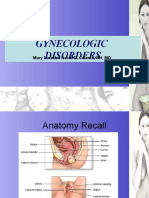
- Gynecologic Disorders: Mary Lourdes Nacel G. Celeste, RN, MDDocument159 paginiGynecologic Disorders: Mary Lourdes Nacel G. Celeste, RN, MDNacel CelesteÎncă nu există evaluări
- Mental Health and Illness: An Epidemiological PerspectiveDocument23 paginiMental Health and Illness: An Epidemiological PerspectiveHervis FantiniÎncă nu există evaluări
- Pediatric and Adolescent Mental HealthDocument33 paginiPediatric and Adolescent Mental HealthHervis FantiniÎncă nu există evaluări
- Put em Down, Take em Out - Knife Fighting - Pentecost, Don PDFDocument31 paginiPut em Down, Take em Out - Knife Fighting - Pentecost, Don PDFStathis Pantzis100% (2)
- Intro To Fungi PresentationDocument22 paginiIntro To Fungi PresentationHervis FantiniÎncă nu există evaluări
- Medically Important FungihandoutDocument55 paginiMedically Important FungihandoutHervis FantiniÎncă nu există evaluări
- Endometrial Cancer: Nancy Wozniak, MDDocument33 paginiEndometrial Cancer: Nancy Wozniak, MDHervis Fantini100% (1)
- Introduction To Color Theory: Color & Rhetorical PurposeDocument21 paginiIntroduction To Color Theory: Color & Rhetorical PurposeHervis FantiniÎncă nu există evaluări
- Solar System FormationDocument43 paginiSolar System FormationHervis FantiniÎncă nu există evaluări
- Colour TheoryDocument29 paginiColour TheoryHervis FantiniÎncă nu există evaluări
- Welcome To The ADocument63 paginiWelcome To The AHervis FantiniÎncă nu există evaluări
- The Solar System: A Fifth Grade ScienceDocument20 paginiThe Solar System: A Fifth Grade ScienceHervis FantiniÎncă nu există evaluări
- CLD FinalDocument17 paginiCLD FinalHervis FantiniÎncă nu există evaluări
- Lab Activity-5Document6 paginiLab Activity-5Kristine MerhanÎncă nu există evaluări
- Viral Infections of The Gastrointestinal Tract and Viral Infections of The Genitourinary SystemDocument14 paginiViral Infections of The Gastrointestinal Tract and Viral Infections of The Genitourinary SystemDARLENE CLAIRE ANDEZAÎncă nu există evaluări
- Cutaneous Squamous Cell CarcinomaDocument43 paginiCutaneous Squamous Cell Carcinomapedrixon123Încă nu există evaluări
- Cerumen Impaction FinalDocument8 paginiCerumen Impaction FinalRose Ann Del MundoÎncă nu există evaluări
- Alter, Klein - 2008 - The Hazards of Blood Transfusion in Historical PerspectiveDocument11 paginiAlter, Klein - 2008 - The Hazards of Blood Transfusion in Historical Perspectivesushmakumari009Încă nu există evaluări
- Mesenchymal Stem Cell Therapeutic Intervention in Covid19Document9 paginiMesenchymal Stem Cell Therapeutic Intervention in Covid19Bala BhaskarÎncă nu există evaluări
- Bionomic of MosquitoesDocument21 paginiBionomic of MosquitoesGani ArlondÎncă nu există evaluări
- Bmjopen 2017 July 7 7 Inline Supplementary Material 1 PDFDocument2 paginiBmjopen 2017 July 7 7 Inline Supplementary Material 1 PDFeyabut1Încă nu există evaluări
- Free Online Mock Test For MHT-CET BIOLOGY PDFDocument28 paginiFree Online Mock Test For MHT-CET BIOLOGY PDFBiologyForMHTCET75% (8)
- Influenza Virus ThesisDocument9 paginiInfluenza Virus Thesisjmvnqiikd100% (2)
- Respiratory ReflectionDocument2 paginiRespiratory ReflectionJennalyn Padua SevillaÎncă nu există evaluări
- ROTAVIRUSDocument13 paginiROTAVIRUSAsma HossainÎncă nu există evaluări
- Livestock and Poultry Production in Nepal and Current Status of Vaccine DevelopmentDocument9 paginiLivestock and Poultry Production in Nepal and Current Status of Vaccine DevelopmentMaheshyepuriÎncă nu există evaluări
- Kulliyyah of Nursing Year 1 Problem-Based Learning: Trigger 1Document17 paginiKulliyyah of Nursing Year 1 Problem-Based Learning: Trigger 1Fitri ZulkifliÎncă nu există evaluări
- ALZENTALDocument2 paginiALZENTALmahgadÎncă nu există evaluări
- Karsinoma Serviks & Vagina SlideshowDocument21 paginiKarsinoma Serviks & Vagina SlideshowFardzli MatjakirÎncă nu există evaluări
- Typhoid FeverDocument13 paginiTyphoid FeverFajar NarakusumaÎncă nu există evaluări
- Linking Dental With Medical Presentation by Dr. Carl Stoel DDSDocument44 paginiLinking Dental With Medical Presentation by Dr. Carl Stoel DDSShivendra Nath TripathiÎncă nu există evaluări
- Rejuvenation Without Medicines - (Authored by Acharya Shriram Sharma)Document47 paginiRejuvenation Without Medicines - (Authored by Acharya Shriram Sharma)Guiding Thoughts- Books by Pandit Shriram Sharma Acharya100% (3)
- MicrobiologyDocument17 paginiMicrobiologykimacol659Încă nu există evaluări
- Evaluation of Antimicrobial Activity of ZITRITIDEDocument16 paginiEvaluation of Antimicrobial Activity of ZITRITIDEednisoÎncă nu există evaluări
- BalatidiumcoliDocument18 paginiBalatidiumcoliakashÎncă nu există evaluări
- 2006 Vento Infection and ThalassemiaDocument8 pagini2006 Vento Infection and ThalassemiarumaishaÎncă nu există evaluări
- Liver FactsDocument26 paginiLiver FactsLiezl SabadoÎncă nu există evaluări
- Cattle Diseases Farmers GuideDocument77 paginiCattle Diseases Farmers GuideDivyajyoti DevaÎncă nu există evaluări
- AFP CalsetDocument1 paginăAFP CalsetModestusÎncă nu există evaluări