S-ar putea să vă placă și
- Problem-based Approach to Gastroenterology and HepatologyDe la EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisÎncă nu există evaluări
- Disorders of Calcium and Phosphate MetabolismDocument20 paginiDisorders of Calcium and Phosphate MetabolismThirupathi Jakkani100% (1)
- Sample Q1Document34 paginiSample Q1Joyeeta Tahseen KhanÎncă nu există evaluări
- Case 1: 25 Yr Old Patient With History of FatigueDocument79 paginiCase 1: 25 Yr Old Patient With History of FatigueMira WryczaÎncă nu există evaluări
- Pentagastrin TestDocument13 paginiPentagastrin TestMustafa KhandgawiÎncă nu există evaluări
- From The Capillaries Into The Capsule ThroughDocument3 paginiFrom The Capillaries Into The Capsule ThroughRashid DayaoÎncă nu există evaluări
- ADR Final1Document10 paginiADR Final1Rubina BisankheÎncă nu există evaluări
- Lecture Notes BacteriologyDocument133 paginiLecture Notes BacteriologyLovely B. AlipatÎncă nu există evaluări
- Anti-Anemia and Hematopoietic Growth FactorsDocument8 paginiAnti-Anemia and Hematopoietic Growth FactorsIsabel CastilloÎncă nu există evaluări
- #3 Pancreatic Hormones & Antidiabetic Drugs 14 PDFDocument14 pagini#3 Pancreatic Hormones & Antidiabetic Drugs 14 PDFOmar BasimÎncă nu există evaluări
- Toxicology Coverage Midterm Exam PDFDocument17 paginiToxicology Coverage Midterm Exam PDFNestor BargioÎncă nu există evaluări
- Therapeutic Drug MonitoringDocument8 paginiTherapeutic Drug MonitoringLourdette TorrefielÎncă nu există evaluări
- Schilling Test: DR - CSBR.Prasad, M.D.Document26 paginiSchilling Test: DR - CSBR.Prasad, M.D.muhammad100% (1)
- Cell TheoryDocument26 paginiCell Theoryحفيظو عبداللهÎncă nu există evaluări
- Horizontal Gene Transfer in BacteriaDocument11 paginiHorizontal Gene Transfer in BacteriaAlejandra arecasÎncă nu există evaluări
- Antihyperlipidemic Drugs: Key Terms Chapter ObjectivesDocument9 paginiAntihyperlipidemic Drugs: Key Terms Chapter ObjectivesSasa AbassÎncă nu există evaluări
- Pharmacognosy: Harmacy Echnicians PharmacyDocument39 paginiPharmacognosy: Harmacy Echnicians PharmacyWaseem Shabbir AhamadÎncă nu există evaluări
- Proper Collection and Preservation of SpecimenDocument6 paginiProper Collection and Preservation of SpecimenDavid SantosÎncă nu există evaluări
- Thyroid Hormones & DrugsDocument51 paginiThyroid Hormones & DrugsSUTHANÎncă nu există evaluări
- Growth HormoneDocument39 paginiGrowth Hormonesalma100% (1)
- Pharm 231: Hospital Pharmacy: Iii. Medication ProfileDocument3 paginiPharm 231: Hospital Pharmacy: Iii. Medication ProfileTESORO Zeus DavidÎncă nu există evaluări
- Bioavailability PK Practice Problems 2013Document2 paginiBioavailability PK Practice Problems 2013Linh PhamÎncă nu există evaluări
- CC Partii&III NotesDocument30 paginiCC Partii&III NotesAnielle Mongaya100% (1)
- Faults Occurring During TrimmingDocument4 paginiFaults Occurring During TrimmingMary Christelle100% (3)
- Pharmacognosy Book of Pharmacy TechnicianDocument138 paginiPharmacognosy Book of Pharmacy TechnicianSabeen MustafaÎncă nu există evaluări
- Digestive System NotesDocument10 paginiDigestive System NotesArchanna VyassÎncă nu există evaluări
- Case Histo PDFDocument19 paginiCase Histo PDFsomayya waliÎncă nu există evaluări
- Carbohydrates Slide-2 PHARM-D, SALUDocument85 paginiCarbohydrates Slide-2 PHARM-D, SALUShahid AhmedÎncă nu există evaluări
- Anticoagulants Used in Blood BankDocument27 paginiAnticoagulants Used in Blood Banklovi bahunÎncă nu există evaluări
- Practice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearDocument44 paginiPractice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearSundarÎncă nu există evaluări
- Clinical Toxicology: Unit I: General Principles of ToxicologyDocument11 paginiClinical Toxicology: Unit I: General Principles of ToxicologyAnnaÎncă nu există evaluări
- Blood Collection VialsDocument26 paginiBlood Collection VialsMunizah MunirÎncă nu există evaluări
- Chapter 42Document3 paginiChapter 42Soc Gerren TuasonÎncă nu există evaluări
- 7 Dengue FeverDocument6 pagini7 Dengue FeverNicole HipolÎncă nu există evaluări
- Pharmaa Topnotch ReviewDocument14 paginiPharmaa Topnotch ReviewArianne Joy C. TamarayÎncă nu există evaluări
- Disorders of Coagulation and Thrombosis NotesDocument16 paginiDisorders of Coagulation and Thrombosis NotesleeÎncă nu există evaluări
- Heme Metabolism PDFDocument19 paginiHeme Metabolism PDFAnonymous jW7BU44ACÎncă nu există evaluări
- Body Fluids-1: Fluid Compartments of The Body Fluid and Electrolyte CompositionDocument33 paginiBody Fluids-1: Fluid Compartments of The Body Fluid and Electrolyte CompositionMan LingÎncă nu există evaluări
- Liver Function TestsDocument3 paginiLiver Function Testssamdaman001Încă nu există evaluări
- Laboratory Tests InterpretationDocument2 paginiLaboratory Tests InterpretationMaria ClaritaÎncă nu există evaluări
- 1335687089.75523 Lab PracticalHematologyManualDocument62 pagini1335687089.75523 Lab PracticalHematologyManualAgustín Manriquez Espinoza0% (1)
- HemoglobinDocument7 paginiHemoglobinNinik Triayu S100% (1)
- Pancreatic Function TestDocument9 paginiPancreatic Function TestAyioKunÎncă nu există evaluări
- Electrolytes: Sodium (Na or Natrium)Document6 paginiElectrolytes: Sodium (Na or Natrium)Emmylou Murillo100% (1)
- PODOPHYLLUMDocument5 paginiPODOPHYLLUMHarish Kakrani100% (1)
- Pharmacology: Drugs That Affect The: Nervous SystemDocument84 paginiPharmacology: Drugs That Affect The: Nervous SystemSameh Saber100% (1)
- Biology MCQS: Mcqs Biology 1St Year & 2Nd Year and For Medical Entry TestDocument58 paginiBiology MCQS: Mcqs Biology 1St Year & 2Nd Year and For Medical Entry TestR.S.H50% (2)
- Ipls & AptsDocument84 paginiIpls & AptsDesalegn TesfayeÎncă nu există evaluări
- Determination of Serum LipidsDocument2 paginiDetermination of Serum LipidsKabo Wale100% (2)
- 152 Experiment 9Document1 pagină152 Experiment 9Earl CañoneroÎncă nu există evaluări
- St. Luke's College of Medicine - William H. Quasha MemorialDocument3 paginiSt. Luke's College of Medicine - William H. Quasha MemorialMavic VillanuevaÎncă nu există evaluări
- 1 IntroDocument5 pagini1 IntroJeanjayannseptoemanÎncă nu există evaluări
- Chapter 5 Endocrinology 1Document53 paginiChapter 5 Endocrinology 1Abubakar JallohÎncă nu există evaluări
- Anemia Its Laboratory DiagnosisDocument146 paginiAnemia Its Laboratory DiagnosisCh M MushahidÎncă nu există evaluări
- Hema I Chapter 12 - ESRDocument30 paginiHema I Chapter 12 - ESRTesfaÎncă nu există evaluări
- Neoplasia: Basic PathologyDocument12 paginiNeoplasia: Basic Pathologyandroid tricksÎncă nu există evaluări
- 6 Ra 1517Document56 pagini6 Ra 1517Jay Andrea Vea Dayuday-IsraelÎncă nu există evaluări
- Blood Physiology: Wang GuoqingDocument89 paginiBlood Physiology: Wang GuoqingFatimah Putri SoniaÎncă nu există evaluări
- Bloodphysiology LECTUREDocument58 paginiBloodphysiology LECTUREShfici AdanÎncă nu există evaluări
- Chapter Blood: RBC Platelet HemostasisDocument89 paginiChapter Blood: RBC Platelet Hemostasisapi-19916399100% (1)
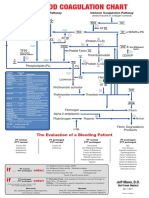
- Blood Clotting ChartDocument1 paginăBlood Clotting ChartBianca SimionescuÎncă nu există evaluări
- Haematology Notes - 3rd EdDocument100 paginiHaematology Notes - 3rd EdSally Brit100% (1)
- MT Activity 1Document18 paginiMT Activity 1Luigie TorresÎncă nu există evaluări
- Especificaciones HumaClot Duo PlusDocument6 paginiEspecificaciones HumaClot Duo PlusMaribelÎncă nu există evaluări
- Anti-Anginal DrugsDocument39 paginiAnti-Anginal Drugspoonam rana100% (1)
- Insert de TP (Thromborel S)Document8 paginiInsert de TP (Thromborel S)Leon Levine80% (5)
- Physiology of PregnancyDocument5 paginiPhysiology of PregnancyLorena Garcia PatiñoÎncă nu există evaluări
- Overview of Platelets: Hematology 2-LaboratortyDocument37 paginiOverview of Platelets: Hematology 2-LaboratortyMiggy PascualÎncă nu există evaluări
- Dailymed NLM Nih Gov Dailymed Fda fdaDrugXsl CFM S E8808230 2c44 44c6 8cab 8f29b6b34051 Type DisplayDocument1 paginăDailymed NLM Nih Gov Dailymed Fda fdaDrugXsl CFM S E8808230 2c44 44c6 8cab 8f29b6b34051 Type DisplayAlex BaleaÎncă nu există evaluări
- Maternal Collapse in Labour WardDocument114 paginiMaternal Collapse in Labour Wardedwardjohnson231080% (5)
- Practical Obstetric Hematology PDFDocument208 paginiPractical Obstetric Hematology PDFSteve CullenÎncă nu există evaluări
- Thromboembolism in The Cat - WSAVA2005 - VINDocument8 paginiThromboembolism in The Cat - WSAVA2005 - VINPet Anjo DiademaÎncă nu există evaluări
- MCQs For LaboratoryDocument42 paginiMCQs For LaboratorySami Khan87% (68)
- Hematology 2 Complete Notes PDFDocument34 paginiHematology 2 Complete Notes PDFVanessa DL100% (1)
- Deep Venous Thrombosis: Practice EssentialsDocument27 paginiDeep Venous Thrombosis: Practice Essentialsphoechoex100% (1)
- Biology B: Pearson Edexcel Level 3 GCEDocument28 paginiBiology B: Pearson Edexcel Level 3 GCEjanaÎncă nu există evaluări
- Shady 11Document96 paginiShady 11Amal AlameenÎncă nu există evaluări
- AntitrombolitikDocument7 paginiAntitrombolitikadityaÎncă nu există evaluări
- The Level of Natural Anticoagulants in Transfusion Dependent Thalassemia Patients in Kelantan Northeastern Malaysia 2329 8790.1000140Document5 paginiThe Level of Natural Anticoagulants in Transfusion Dependent Thalassemia Patients in Kelantan Northeastern Malaysia 2329 8790.1000140kusumahpratiwiÎncă nu există evaluări
- Lquiplastine - PTDocument2 paginiLquiplastine - PTm sdÎncă nu există evaluări
- F4 BIO2 Year End 2022 AnswersDocument9 paginiF4 BIO2 Year End 2022 AnswersArsyad DanishÎncă nu există evaluări
- Bromelain: A Literature Review and Discussion of Its Therapeutic ApplicationsDocument16 paginiBromelain: A Literature Review and Discussion of Its Therapeutic ApplicationsPaolo MilanÎncă nu există evaluări
- Biology 12 - Chapter 11 - Blood - Chapter Notes: Here Is A Micrographs Showing Formed Elements in Human BloodDocument7 paginiBiology 12 - Chapter 11 - Blood - Chapter Notes: Here Is A Micrographs Showing Formed Elements in Human BloodChan KarlokÎncă nu există evaluări
- Fisiopatologia Del PolitraumaDocument19 paginiFisiopatologia Del PolitraumaYuen WcÎncă nu există evaluări
- Bleeding Disorders InvestigationDocument2 paginiBleeding Disorders InvestigationVarshaa BharathiÎncă nu există evaluări
- Heparin Sodium Injection, USP: RX Only DescriptionDocument29 paginiHeparin Sodium Injection, USP: RX Only DescriptionArchie TobiasÎncă nu există evaluări
- Vascular Surgery MCQsDocument66 paginiVascular Surgery MCQsJaclyn Mcdonald86% (22)
- Immunology ExamsDocument120 paginiImmunology ExamsThanuja SureshÎncă nu există evaluări
- Assessment Hema PDFDocument9 paginiAssessment Hema PDFAnne MorenoÎncă nu există evaluări
- Adsorbed PlasmaDocument3 paginiAdsorbed PlasmaDevi OktaviannyÎncă nu există evaluări