S-ar putea să vă placă și
- Boast 1 - Fragility Hip Fractures PDFDocument1 paginăBoast 1 - Fragility Hip Fractures PDFSam BarnesÎncă nu există evaluări
- AnestesiaDocument13 paginiAnestesialuisfernandoamaya89Încă nu există evaluări
- People With Spinal Cord Injury in Indonesia: Ountry EportDocument4 paginiPeople With Spinal Cord Injury in Indonesia: Ountry EportAnindira RustandiÎncă nu există evaluări
- Helix Alliance - Resume (Dr. Appukutty Manickam (Kumar) ) - 1Document6 paginiHelix Alliance - Resume (Dr. Appukutty Manickam (Kumar) ) - 1indo 5SÎncă nu există evaluări
- ANZ Journal of Surgery - 2001 - Rankin - Costs of Accessing Surgical Specialists by Rural and Remote ResidentsDocument4 paginiANZ Journal of Surgery - 2001 - Rankin - Costs of Accessing Surgical Specialists by Rural and Remote ResidentsJeff CrocombeÎncă nu există evaluări
- Original Research Paper Neurosurgery: Epidemiology of Head Injury-Level 1 Taei Centre StudyDocument6 paginiOriginal Research Paper Neurosurgery: Epidemiology of Head Injury-Level 1 Taei Centre StudyArjun CVÎncă nu există evaluări
- Iadt03i5p328 PDFDocument10 paginiIadt03i5p328 PDFSanju HasiniÎncă nu există evaluări
- Shetty, A., & Ravendra, U.S. (2015) - Anesthesia For Day Care Surgery. Nitte University Journal of Health Science, Vol. 5, No. 2, 97-103Document7 paginiShetty, A., & Ravendra, U.S. (2015) - Anesthesia For Day Care Surgery. Nitte University Journal of Health Science, Vol. 5, No. 2, 97-103kadek gunadiÎncă nu există evaluări
- 9.2 Redesigning Trauma OperationsDocument6 pagini9.2 Redesigning Trauma OperationsanuragÎncă nu există evaluări
- Acut Care Surgery in Rural SVARASDocument37 paginiAcut Care Surgery in Rural SVARASJOHANES BERECHMANS PRANOTO RUMARATUÎncă nu există evaluări
- Telemedicine in SurgeryDocument18 paginiTelemedicine in SurgeryIpseet Mishra100% (1)
- Point of Care Ultrasound: The Critical Imaging Tool For The Critically UnwellDocument10 paginiPoint of Care Ultrasound: The Critical Imaging Tool For The Critically UnwellOswaldo OrtizÎncă nu există evaluări
- Implementation of The Modified Canadian C Spine Rule by ParamedicsDocument10 paginiImplementation of The Modified Canadian C Spine Rule by Paramedicscarper454Încă nu există evaluări
- Best Practices in The Management of Orthopaedic Trauma: Acs TqipDocument38 paginiBest Practices in The Management of Orthopaedic Trauma: Acs TqipandhiyatnoermandakaÎncă nu există evaluări
- DR Nadia AhmadDocument4 paginiDR Nadia AhmadNadia AhmadÎncă nu există evaluări
- Laboratory Activity 3 - HIS Lab - Classification of Health Care FacilitiesDocument5 paginiLaboratory Activity 3 - HIS Lab - Classification of Health Care FacilitiesCaissa Andrea Beatrice BaylenÎncă nu există evaluări
- Operating Room ProcedureDocument6 paginiOperating Room ProcedureleviÎncă nu există evaluări
- 68 2023 Article 2288Document7 pagini68 2023 Article 2288Su Ling ShihÎncă nu există evaluări
- 118 PrelimDocument18 pagini118 PrelimAudrey Ann AcobÎncă nu există evaluări
- Neurotrauma Rural Guidelines 2edDocument27 paginiNeurotrauma Rural Guidelines 2edAldion ZericoÎncă nu există evaluări
- HPD Group 10Document20 paginiHPD Group 10Shruti SinghÎncă nu există evaluări
- Nurses Knowledge Toward Cast Complications in Orthopedic Ward at Al-Najaf AL-Ashraf HospitalsDocument7 paginiNurses Knowledge Toward Cast Complications in Orthopedic Ward at Al-Najaf AL-Ashraf HospitalsZilbran BerontaxÎncă nu există evaluări
- Hospital Training ReportDocument75 paginiHospital Training ReportABINAYA80% (5)
- CV. Dr. Erwadi.Document2 paginiCV. Dr. Erwadi.Erwadi ErwadiÎncă nu există evaluări
- Naukri VenkataSriTejaGarimella (6y 6m)Document3 paginiNaukri VenkataSriTejaGarimella (6y 6m)VTekis ConsultingÎncă nu există evaluări
- Vascular Disease 2018: The Provision of Services For Patients WithDocument48 paginiVascular Disease 2018: The Provision of Services For Patients WithcindyÎncă nu există evaluări
- Sample Nurse Aide ResumeDocument2 paginiSample Nurse Aide ResumeMayta Bacud RamosÎncă nu există evaluări
- Needle Stik InjuryDocument6 paginiNeedle Stik Injurywijaya ajaaÎncă nu există evaluări
- 268 2014 Article 2663 PDFDocument12 pagini268 2014 Article 2663 PDFAnonymous 1nMTZWmzÎncă nu există evaluări
- Referral HospitalDocument10 paginiReferral HospitalSundaramoorthy KaliappanÎncă nu există evaluări
- Anesthesia For Off-Floor Dental and Oral Surgery: ReviewDocument7 paginiAnesthesia For Off-Floor Dental and Oral Surgery: ReviewDariana JDÎncă nu există evaluări
- Anesthesia Website 04jan2019Document18 paginiAnesthesia Website 04jan2019Pranav PujariÎncă nu există evaluări
- Guidelines For A Sustainable Specialist Neurosurgical Service-1Document5 paginiGuidelines For A Sustainable Specialist Neurosurgical Service-1davidrahman5Încă nu există evaluări
- Peran Perawat Dalam Antisipasi Dan Penanganan Keadaan Gawat DaruratDocument43 paginiPeran Perawat Dalam Antisipasi Dan Penanganan Keadaan Gawat DaruratId C4rdÎncă nu există evaluări
- Ms Ellaine Boo Role of Trauma NursingDocument35 paginiMs Ellaine Boo Role of Trauma NursingBrunoÎncă nu există evaluări
- Wellington Brochure PDFDocument9 paginiWellington Brochure PDFgorill4Încă nu există evaluări
- Anaesthetic Considerations in Polytrauma PatientsDocument8 paginiAnaesthetic Considerations in Polytrauma PatientsMileidys LopezÎncă nu există evaluări
- BLK BrochureDocument16 paginiBLK Brochurearshad khanÎncă nu există evaluări
- Service Spec Spinal Cord Injury Services All AgesDocument19 paginiService Spec Spinal Cord Injury Services All AgesKenneth KalyangoÎncă nu există evaluări
- Telemedicine in IndiaDocument6 paginiTelemedicine in IndiaSumathy YsÎncă nu există evaluări
- Dr. Rajeev Lochan Tailor - ResumeDocument2 paginiDr. Rajeev Lochan Tailor - ResumecpvetbackendÎncă nu există evaluări
- Guidelines Limb Salvage OsteosarcomaDocument9 paginiGuidelines Limb Salvage OsteosarcomaZunnoorain RaeÎncă nu există evaluări
- Group13casestudy 220204162727Document26 paginiGroup13casestudy 220204162727Abhi SharmaÎncă nu există evaluări
- Welcome To Your International: Medical and Travel Assistance ServiceDocument2 paginiWelcome To Your International: Medical and Travel Assistance ServiceAntoineÎncă nu există evaluări
- MVT Brochure - v6 CompressedDocument20 paginiMVT Brochure - v6 CompressedBiswajeet GangulyÎncă nu există evaluări
- The Principle of Traction and The Application of Lower Limb SkinDocument4 paginiThe Principle of Traction and The Application of Lower Limb SkinMarina UlfaÎncă nu există evaluări
- Unit 3Document7 paginiUnit 3luciagarper1Încă nu există evaluări
- District Hospital Standards PDFDocument23 paginiDistrict Hospital Standards PDFsurbhi aggarwalÎncă nu există evaluări
- Critical Care Set UpDocument33 paginiCritical Care Set UpSam TullyÎncă nu există evaluări
- Score Predicting The Need For Hospitalization in Scorpion EnvenomationDocument7 paginiScore Predicting The Need For Hospitalization in Scorpion EnvenomationWalaa YousefÎncă nu există evaluări
- Petrus Nnolim CVDocument5 paginiPetrus Nnolim CVagni.nnolimÎncă nu există evaluări
- Emailing Manual of Large Animal Surgical TechniquesDocument68 paginiEmailing Manual of Large Animal Surgical TechniquesNote FormÎncă nu există evaluări
- Apparentship Report (By WU-AHN Students)Document10 paginiApparentship Report (By WU-AHN Students)Mitiku TekaÎncă nu există evaluări
- Providing A Lifeline For Rural DoctorsDocument2 paginiProviding A Lifeline For Rural Doctorsbibin babuÎncă nu există evaluări
- Stroke Unit Position Paper FINALDocument4 paginiStroke Unit Position Paper FINALsatyagraha84Încă nu există evaluări
- Curriculum Vitae: Name Date of Birth Nationality GMC NumberDocument13 paginiCurriculum Vitae: Name Date of Birth Nationality GMC NumberRazor GGÎncă nu există evaluări
- Anaesthetics ST1 ST2 1 February 2007 - 4960Document10 paginiAnaesthetics ST1 ST2 1 February 2007 - 4960Trevor SoarÎncă nu există evaluări
- Eshraga Esress :co. Esra AbdelgadirDocument3 paginiEshraga Esress :co. Esra Abdelgadirmohammed.hafr1999Încă nu există evaluări
- Wound Management for the Advanced PractitionerDe la EverandWound Management for the Advanced PractitionerEvaluare: 2 din 5 stele2/5 (2)
- Blockmate: A Practical Guide for Ultrasound Guided Regional AnaesthesiaDe la EverandBlockmate: A Practical Guide for Ultrasound Guided Regional AnaesthesiaArunangshu ChakrabortyÎncă nu există evaluări
- Ms Ellaine Boo Role of Trauma NursingDocument35 paginiMs Ellaine Boo Role of Trauma NursingBrunoÎncă nu există evaluări
- Physiology and Pathology of Physical and Psychological StressDocument60 paginiPhysiology and Pathology of Physical and Psychological StressBrunoÎncă nu există evaluări
- Prof DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesDocument42 paginiProf DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesBrunoÎncă nu există evaluări
- DR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonDocument25 paginiDR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonBrunoÎncă nu există evaluări
- DR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsDocument32 paginiDR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsBruno100% (1)
- Prof - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenDocument40 paginiProf - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenBrunoÎncă nu există evaluări
- DR - Ramana Rao Pre-Hospital Services in Tamil NaduDocument73 paginiDR - Ramana Rao Pre-Hospital Services in Tamil NaduBrunoÎncă nu există evaluări
- Mrs. Sulochana (RGGGH) Current Status of Trauma Nursing in TNDocument11 paginiMrs. Sulochana (RGGGH) Current Status of Trauma Nursing in TNBrunoÎncă nu există evaluări
- DR - Joseph Mathew: Trauma Units and Team WorkDocument39 paginiDR - Joseph Mathew: Trauma Units and Team WorkBrunoÎncă nu există evaluări
- Hub and Spoke Model For STEMI Management - Tamil Nadu ModelDocument16 paginiHub and Spoke Model For STEMI Management - Tamil Nadu ModelBrunoÎncă nu există evaluări
- Prof Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryDocument37 paginiProf Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryBrunoÎncă nu există evaluări
- Neurosurgeon For A Social CauseDocument55 paginiNeurosurgeon For A Social CauseBrunoÎncă nu există evaluări
- DR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianDocument36 paginiDR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianBruno100% (1)
- TAEI NTRI WorkshopDocument16 paginiTAEI NTRI WorkshopBrunoÎncă nu există evaluări
- How Tamil Nadu Eradicated Organ SaleDocument108 paginiHow Tamil Nadu Eradicated Organ SaleBrunoÎncă nu există evaluări
- Prof DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsDocument36 paginiProf DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsBrunoÎncă nu există evaluări
- Prof DR Amit Gupta AITSC Trauma Registry & Trauma Quality Improvement in IndiaDocument77 paginiProf DR Amit Gupta AITSC Trauma Registry & Trauma Quality Improvement in IndiaBruno50% (2)
- Ian Patrick Pre-Hospital Systems in Australia Key Components of The Pre-Hospital System in Australia and Best Buys For Tamil NaduDocument26 paginiIan Patrick Pre-Hospital Systems in Australia Key Components of The Pre-Hospital System in Australia and Best Buys For Tamil NaduBrunoÎncă nu există evaluări
- Mr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusDocument25 paginiMr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusBruno100% (1)
- Prof DR Peter Cameron Measuring The Quality of Trauma Systems and In-Hospital Trauma CareDocument46 paginiProf DR Peter Cameron Measuring The Quality of Trauma Systems and In-Hospital Trauma CareBrunoÎncă nu există evaluări
- Why Tamil Nadu Model Works Better in Eradicating Organ SaleDocument52 paginiWhy Tamil Nadu Model Works Better in Eradicating Organ SaleBrunoÎncă nu există evaluări
- Doctors' Role in Tackling Organ TradeDocument70 paginiDoctors' Role in Tackling Organ TradeBrunoÎncă nu există evaluări
- DR - Darez Ahamed Vision For Tamil NaduDocument6 paginiDR - Darez Ahamed Vision For Tamil NaduBrunoÎncă nu există evaluări
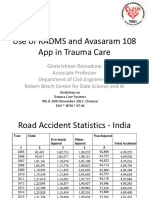
- Prof Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareDocument21 paginiProf Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareBrunoÎncă nu există evaluări
- Neurology, Neurosurgery MCQ PointsDocument32 paginiNeurology, Neurosurgery MCQ PointsBruno86% (7)
- TN Gazette 47 of 2013 Part VI Section 4Document84 paginiTN Gazette 47 of 2013 Part VI Section 4BrunoÎncă nu există evaluări
- AR Rahman PDFDocument405 paginiAR Rahman PDFPitchai BalaÎncă nu există evaluări
- NEET PG 2013 Rank List of Eligible CandidatesDocument256 paginiNEET PG 2013 Rank List of Eligible CandidatesBruno75% (8)
- HMIS - Health Management Information System - Government of Tamil NaduDocument12 paginiHMIS - Health Management Information System - Government of Tamil NaduBruno100% (1)
- BTEC - Assignment - Brief A2 Unit 21 2Document3 paginiBTEC - Assignment - Brief A2 Unit 21 2Dariusz LangeÎncă nu există evaluări
- Research Paper FinalDocument12 paginiResearch Paper Finalapi-582867034Încă nu există evaluări
- Reducing Negativity in A WorkplaceDocument12 paginiReducing Negativity in A WorkplaceAna Jane Morales CasaclangÎncă nu există evaluări
- Medical Informatics - Concepts, Methodologies, Tools, and Applications (Premier Reference Source) (PDFDrive)Document2.593 paginiMedical Informatics - Concepts, Methodologies, Tools, and Applications (Premier Reference Source) (PDFDrive)tinanoÎncă nu există evaluări
- Medical Equipment Quality Assurance (Tobey Clark, U Vermont)Document151 paginiMedical Equipment Quality Assurance (Tobey Clark, U Vermont)MelissaBarriosUrcia100% (2)
- Bulletin 201215 (HTML Edition)Document128 paginiBulletin 201215 (HTML Edition)DonnieÎncă nu există evaluări
- Claims FAQDocument4 paginiClaims FAQSaiCharan GarimellaÎncă nu există evaluări
- Process Safety and Environmental Protection 2009 Volume 87, Number 1Document2 paginiProcess Safety and Environmental Protection 2009 Volume 87, Number 1jenanboyzÎncă nu există evaluări
- Maria MontessoriDocument2 paginiMaria MontessoriGiulia SpadariÎncă nu există evaluări
- SP - Sindy MilaDocument2 paginiSP - Sindy MilaSindy MelindaÎncă nu există evaluări
- A Village Square Lesson PlanDocument4 paginiA Village Square Lesson PlanShivaniÎncă nu există evaluări
- Medimanet: Recent Achievements in Drug Library and Safety TechnologyDocument2 paginiMedimanet: Recent Achievements in Drug Library and Safety TechnologyDiani VargasÎncă nu există evaluări
- MIP17 - HSE - PP - 001 Environment Management Plan (EMP) 2021 REV 3Document40 paginiMIP17 - HSE - PP - 001 Environment Management Plan (EMP) 2021 REV 3AmeerHamzaWarraichÎncă nu există evaluări
- Shofa Aji Setyoko (N101 12 051)Document4 paginiShofa Aji Setyoko (N101 12 051)ShofaajiÎncă nu există evaluări
- LAS10 Week 4 7 2nd QuarterDocument4 paginiLAS10 Week 4 7 2nd QuarterGleamor DaagÎncă nu există evaluări
- Kacee-New ResumeDocument4 paginiKacee-New Resumeapi-678307618Încă nu există evaluări
- Neuro Lymphatic MassageDocument2 paginiNeuro Lymphatic Massagewolfgangl70Încă nu există evaluări
- German Marine Agencies Inc Vs NLRC 142049 JanuaryDocument14 paginiGerman Marine Agencies Inc Vs NLRC 142049 JanuaryJennyÎncă nu există evaluări
- Cancer-Relatedfatiguein Cancersurvivorship: Chidinma C. Ebede,, Yongchang Jang,, Carmen P. EscalanteDocument13 paginiCancer-Relatedfatiguein Cancersurvivorship: Chidinma C. Ebede,, Yongchang Jang,, Carmen P. EscalanteMahdhun ShiddiqÎncă nu există evaluări
- Surgical Handicraft Manual For Surgical Residents 2015 PDFDocument295 paginiSurgical Handicraft Manual For Surgical Residents 2015 PDFNamerahN100% (3)
- The Intentional Application of Humor With CKD PatientsDocument8 paginiThe Intentional Application of Humor With CKD PatientsKaryn BuxmanÎncă nu există evaluări
- Microbiome Labs Total Gut RestorationDocument2 paginiMicrobiome Labs Total Gut RestorationKrishna DasÎncă nu există evaluări
- HSE Covid-19 Doffing CoverallDocument1 paginăHSE Covid-19 Doffing Coveralliq_dianaÎncă nu există evaluări
- Miranda Miracell NewDocument2 paginiMiranda Miracell NewPablo FaldutiÎncă nu există evaluări
- The Superheroes of PharmaDocument13 paginiThe Superheroes of PharmaMPAÎncă nu există evaluări
- InterbarkadaDocument8 paginiInterbarkadaJay Vincent DiamanteÎncă nu există evaluări
- Karyotype WorksheetDocument4 paginiKaryotype WorksheetKellieM.8406Încă nu există evaluări
- Journal Club: A Step Towards Evidence Based Practice: January 2011Document6 paginiJournal Club: A Step Towards Evidence Based Practice: January 2011Jommy ChawalaÎncă nu există evaluări
- GayDocument15 paginiGayjulyerwanni100% (2)
- Risk Management in Military AviationDocument16 paginiRisk Management in Military AviationSp AndaÎncă nu există evaluări