S-ar putea să vă placă și
- Neurology, Neurosurgery MCQ PointsDocument32 paginiNeurology, Neurosurgery MCQ PointsBruno86% (7)
- Case Report Supracondylar Fracture of Right FemurDocument37 paginiCase Report Supracondylar Fracture of Right FemurSri Mahtufa Riski100% (1)
- COCONUT OIL 101 Miraculous Coconut Oil Benefits Cures Uses and Remedies by Victoria Lane PDFDocument22 paginiCOCONUT OIL 101 Miraculous Coconut Oil Benefits Cures Uses and Remedies by Victoria Lane PDFedwinw18Încă nu există evaluări
- Lung CancerDocument8 paginiLung CancerRosalenlen LlanezaÎncă nu există evaluări
- Lower Limb ProstheticsDocument28 paginiLower Limb ProstheticsSomu VictorÎncă nu există evaluări
- First Aid NotesDocument13 paginiFirst Aid NotesVian ArccenioÎncă nu există evaluări
- 22ca ColonDocument21 pagini22ca ColonDrVishal BhattÎncă nu există evaluări
- Perioperative Care Plan: AGE MedicationsDocument3 paginiPerioperative Care Plan: AGE MedicationsDian Cahyo WibowoÎncă nu există evaluări
- Adoption: Legal DefinitionDocument8 paginiAdoption: Legal Definitionsharon victoria mendezÎncă nu există evaluări
- Basic Principles of Local Flap in Plastic SurgeryDocument118 paginiBasic Principles of Local Flap in Plastic SurgerySiti Fildzah NadhilahÎncă nu există evaluări
- Fracture Femur: Presented By: Erin Triana Ronald TejoprayitnoDocument29 paginiFracture Femur: Presented By: Erin Triana Ronald Tejoprayitnoronald_tejopray742Încă nu există evaluări
- Guidelines For Management of Head InjuryDocument18 paginiGuidelines For Management of Head InjuryChellamani UmakanthanÎncă nu există evaluări
- 1 - Case HistoryDocument47 pagini1 - Case HistoryAishwarya S. NairÎncă nu există evaluări
- EMS Burn Management PDFDocument30 paginiEMS Burn Management PDFRaymond Sitanaja0% (1)
- Burns First AidDocument23 paginiBurns First AidBinanda MoirangthemÎncă nu există evaluări
- OsteosarcomaDocument25 paginiOsteosarcomaChaitra Mahesh67% (3)
- First Aid Teaching FormatDocument23 paginiFirst Aid Teaching FormatMichaelÎncă nu există evaluări
- Hospital Disclosure PolicyDocument10 paginiHospital Disclosure Policyvks7876Încă nu există evaluări
- NEET PG 2013 Rank List of Eligible CandidatesDocument256 paginiNEET PG 2013 Rank List of Eligible CandidatesBruno75% (8)
- Organ Donation Act of 1991Document10 paginiOrgan Donation Act of 1991Dayledaniel Sorveto100% (1)
- 11 Uterine CancerDocument43 pagini11 Uterine Cancerclaire yowsÎncă nu există evaluări
- Endometrial Malignancies 1Document41 paginiEndometrial Malignancies 1jerrydanfordfxÎncă nu există evaluări
- Dha LastDocument197 paginiDha LastCarlos Vidal Tudela89% (27)
- Ear DisordersDocument10 paginiEar DisordersPatzie MolinaÎncă nu există evaluări
- Day Care SurgeryDocument5 paginiDay Care SurgeryazharmoÎncă nu există evaluări
- EMT Webinar 20 06 17Document30 paginiEMT Webinar 20 06 17Zahra Muslimah-Nuryati ZahraÎncă nu există evaluări
- Bullying in Residency Training ArticleDocument10 paginiBullying in Residency Training ArticleFiryal BalushiÎncă nu există evaluări
- Supracondylar Fractures: Bui Thi Huong Group 6-Y3B Saint Paul HospitalDocument24 paginiSupracondylar Fractures: Bui Thi Huong Group 6-Y3B Saint Paul HospitalHườngÎncă nu există evaluări
- Human Organ Tranplantation ActDocument6 paginiHuman Organ Tranplantation ActFrank NobodÎncă nu există evaluări
- Proceedings of The National Workshop On INTRODUCING YOGA IN MEDICAL CURRICULUMDocument76 paginiProceedings of The National Workshop On INTRODUCING YOGA IN MEDICAL CURRICULUMYogacharya Dr Ananda Balayogi Bhavanani0% (1)
- Virtual SurgeryDocument22 paginiVirtual SurgeryMounika Surapaneni100% (1)
- Panel DiscussionDocument5 paginiPanel DiscussionArpit MehraÎncă nu există evaluări
- Prof Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryDocument37 paginiProf Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryBrunoÎncă nu există evaluări
- Management of HIV InfectionDocument29 paginiManagement of HIV InfectionHuda HamoudaÎncă nu există evaluări
- Emergency Rescue and TransferDocument35 paginiEmergency Rescue and TransferGavinKarl MianabanataoÎncă nu există evaluări
- Surgery, General, Wounds and Wound HealingDocument15 paginiSurgery, General, Wounds and Wound HealingRhazes78100% (1)
- Live Young, Think Young, Be Young: . . . At Any AgeDe la EverandLive Young, Think Young, Be Young: . . . At Any AgeEvaluare: 5 din 5 stele5/5 (1)
- BTLS TraumaDocument41 paginiBTLS TraumaArif Dika MahendraÎncă nu există evaluări
- Lung CancerDocument9 paginiLung CancerMahmood SaeedÎncă nu există evaluări
- Anchoring Script BnakingDocument5 paginiAnchoring Script BnakingFatema Tuz JohooraÎncă nu există evaluări
- IV Site AssessmentDocument1 paginăIV Site AssessmentalkhaqaniÎncă nu există evaluări
- Preoperative ChecklistDocument3 paginiPreoperative Checklistraj1969Încă nu există evaluări
- Basic Infection Prevention and Control For Hospital Staff and Healthcare ProvidersDocument60 paginiBasic Infection Prevention and Control For Hospital Staff and Healthcare ProvidersaringkinkingÎncă nu există evaluări
- Cauti Prevention - UpdatedDocument25 paginiCauti Prevention - Updatedapi-340518242Încă nu există evaluări
- Chapter 01 PDFDocument14 paginiChapter 01 PDFMeera KrishnanÎncă nu există evaluări
- Trauma CareDocument34 paginiTrauma CareGovindarajan HariharanÎncă nu există evaluări
- Computer Aided Maxillofacial Surgery: (With Human Anatomic Specimens)Document4 paginiComputer Aided Maxillofacial Surgery: (With Human Anatomic Specimens)copyourpairÎncă nu există evaluări
- Newsletter Volume 4Document8 paginiNewsletter Volume 4Deepak Agrawal100% (1)
- Ems Pak 1997Document4 paginiEms Pak 1997Tri Monarita JohanÎncă nu există evaluări
- TAEI NTRI WorkshopDocument16 paginiTAEI NTRI WorkshopBrunoÎncă nu există evaluări
- 7 Steps Patient Safety PDFDocument58 pagini7 Steps Patient Safety PDFDanissa Fidia PuteriÎncă nu există evaluări
- Proposed Scheme of Service For EMTs in KenyaDocument19 paginiProposed Scheme of Service For EMTs in KenyaBrian Beauttah67% (3)
- Prof DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsDocument36 paginiProf DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsBrunoÎncă nu există evaluări
- Image Segmentation Methods and Edge Dete PDFDocument11 paginiImage Segmentation Methods and Edge Dete PDFjosenaranjoÎncă nu există evaluări
- Applied Nursing Research: Mary Louise Kanaskie, PHD, RN-BC, Aocn, Cynthia Snyder, MSN, RNDocument7 paginiApplied Nursing Research: Mary Louise Kanaskie, PHD, RN-BC, Aocn, Cynthia Snyder, MSN, RNGabriella CsernákÎncă nu există evaluări
- Toward An Ultrasound Curriculum For Critical Care Medicine PDFDocument15 paginiToward An Ultrasound Curriculum For Critical Care Medicine PDFBasilia CahuichÎncă nu există evaluări
- Spinal Cord Independence Measure III (SCIM III) : Toolkit ForDocument24 paginiSpinal Cord Independence Measure III (SCIM III) : Toolkit ForLisa NurhasanahÎncă nu există evaluări
- Muresan 2020Document8 paginiMuresan 2020Aljabouri AbdelwahabÎncă nu există evaluări
- Briefings and Debriefings in The Operating Room: The VA ExperienceDocument35 paginiBriefings and Debriefings in The Operating Room: The VA Experienced40sithuiÎncă nu există evaluări
- Issue 6Document8 paginiIssue 6Deepak AgrawalÎncă nu există evaluări
- 1 s2.0 S2351978915005600 MainDocument8 pagini1 s2.0 S2351978915005600 MainhilmaÎncă nu există evaluări
- NHS 2019 Transforming - Imaging - ServicesDocument55 paginiNHS 2019 Transforming - Imaging - ServicesShirley SpenceÎncă nu există evaluări
- Assis 2017Document19 paginiAssis 2017widyadariÎncă nu există evaluări
- Ergonomic Issues For Health Care - Back Injuries: BSO Course 3/2002Document31 paginiErgonomic Issues For Health Care - Back Injuries: BSO Course 3/2002putrioktarianiÎncă nu există evaluări
- Development of The Patient Safety Incident Management System (DPSIMS) : Stakeholder UpdateDocument18 paginiDevelopment of The Patient Safety Incident Management System (DPSIMS) : Stakeholder UpdateDante820Încă nu există evaluări
- Community Health SkillsDocument1 paginăCommunity Health Skillsapi-383910447Încă nu există evaluări
- Physiology and Pathology of Physical and Psychological StressDocument60 paginiPhysiology and Pathology of Physical and Psychological StressBrunoÎncă nu există evaluări
- DR - Joseph Mathew: Trauma Units and Team WorkDocument39 paginiDR - Joseph Mathew: Trauma Units and Team WorkBrunoÎncă nu există evaluări
- Prof - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenDocument40 paginiProf - Dr.Indumathy Santhanam (ICH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of ChildrenBrunoÎncă nu există evaluări
- DR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonDocument25 paginiDR - Raja S Vignesh (Thoothukudi Medical College) in Hospital Care of Patient by NeurosurgeonBrunoÎncă nu există evaluări
- Ms Ellaine Boo Role of Trauma NursingDocument35 paginiMs Ellaine Boo Role of Trauma NursingBrunoÎncă nu există evaluări
- DR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsDocument32 paginiDR - Rajesh CMO (RGGGH) In-Hospital Care of Trauma Patients in Tamil Nadu - Current Systems For Management of AdultsBruno100% (1)
- Prof DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesDocument42 paginiProf DR Mark Fitzgerald Integrated In-Hospital Trauma Care - Building Blocks That Save LivesBrunoÎncă nu există evaluări
- DR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianDocument36 paginiDR - Thambaiah (Cuddalore GH) in Hospital Care of Patients by OrthopaedicianBruno100% (1)
- TAEI NTRI WorkshopDocument16 paginiTAEI NTRI WorkshopBrunoÎncă nu există evaluări
- Hub and Spoke Model For STEMI Management - Tamil Nadu ModelDocument16 paginiHub and Spoke Model For STEMI Management - Tamil Nadu ModelBrunoÎncă nu există evaluări
- Prof Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryDocument37 paginiProf Venkatesh Balasubramanian Current State Road Accident Database and Requirements For Integration of A Trauma RegistryBrunoÎncă nu există evaluări
- Mrs. Sulochana (RGGGH) Current Status of Trauma Nursing in TNDocument11 paginiMrs. Sulochana (RGGGH) Current Status of Trauma Nursing in TNBrunoÎncă nu există evaluări
- Prof DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsDocument36 paginiProf DR Mark Fitzgerald What Is A Trauma System and Trauma System ComponentsBrunoÎncă nu există evaluări
- DR - Ramana Rao Pre-Hospital Services in Tamil NaduDocument73 paginiDR - Ramana Rao Pre-Hospital Services in Tamil NaduBrunoÎncă nu există evaluări
- Mr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusDocument25 paginiMr. Dayanand Kataria, IAS Transport Commissioner Road Safety StatusBruno100% (1)
- DR - Darez Ahamed Vision For Tamil NaduDocument6 paginiDR - Darez Ahamed Vision For Tamil NaduBrunoÎncă nu există evaluări
- Prof DR Peter Cameron Measuring The Quality of Trauma Systems and In-Hospital Trauma CareDocument46 paginiProf DR Peter Cameron Measuring The Quality of Trauma Systems and In-Hospital Trauma CareBrunoÎncă nu există evaluări
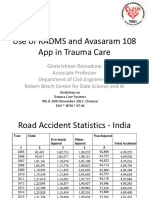
- Prof Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareDocument21 paginiProf Gita Krishnan Ramadurai Use of RADAMS and 108 Avasaram App in Trauma CareBrunoÎncă nu există evaluări
- DR Joseph Mathew Designation of Trauma Hospitals in A Trauma SystemDocument29 paginiDR Joseph Mathew Designation of Trauma Hospitals in A Trauma SystemBrunoÎncă nu există evaluări
- Ian Patrick Pre-Hospital Systems in Australia Key Components of The Pre-Hospital System in Australia and Best Buys For Tamil NaduDocument26 paginiIan Patrick Pre-Hospital Systems in Australia Key Components of The Pre-Hospital System in Australia and Best Buys For Tamil NaduBrunoÎncă nu există evaluări
- Doctors' Role in Tackling Organ TradeDocument70 paginiDoctors' Role in Tackling Organ TradeBrunoÎncă nu există evaluări
- How Tamil Nadu Eradicated Organ SaleDocument108 paginiHow Tamil Nadu Eradicated Organ SaleBrunoÎncă nu există evaluări
- Why Tamil Nadu Model Works Better in Eradicating Organ SaleDocument52 paginiWhy Tamil Nadu Model Works Better in Eradicating Organ SaleBrunoÎncă nu există evaluări
- AR Rahman PDFDocument405 paginiAR Rahman PDFPitchai BalaÎncă nu există evaluări
- Neurosurgeon For A Social CauseDocument55 paginiNeurosurgeon For A Social CauseBrunoÎncă nu există evaluări
- TN Gazette 47 of 2013 Part VI Section 4Document84 paginiTN Gazette 47 of 2013 Part VI Section 4BrunoÎncă nu există evaluări
- HMIS - Health Management Information System - Government of Tamil NaduDocument12 paginiHMIS - Health Management Information System - Government of Tamil NaduBruno100% (1)
- 2ton Steel 56.8gDocument4 pagini2ton Steel 56.8gYasir AzmatÎncă nu există evaluări
- Glimpse of My ResearchDocument4 paginiGlimpse of My Researchमनोज जैनÎncă nu există evaluări
- Rumah Sakit Bhakti MuliaDocument3 paginiRumah Sakit Bhakti MuliaSarachanda SallyÎncă nu există evaluări
- Gynecological LaparosDocument32 paginiGynecological LaparosYosef Dwi Cahyadi Salan100% (1)
- Inborn Errors or MetabolismDocument25 paginiInborn Errors or MetabolismSamdiSutantoÎncă nu există evaluări
- 3rd Care of The Critically Ill Surgical Patient PDFDocument273 pagini3rd Care of The Critically Ill Surgical Patient PDFPavitra RamasamyÎncă nu există evaluări
- Pelvis Frozen EnglishDocument3 paginiPelvis Frozen EnglishPetar PribicÎncă nu există evaluări
- Momordica Cochinchinensis, Rosa Roxburghii, Wolfberry, and Sea Buckthorn-Highly Nutritional Fruits Supported by Tradition and ScienceDocument8 paginiMomordica Cochinchinensis, Rosa Roxburghii, Wolfberry, and Sea Buckthorn-Highly Nutritional Fruits Supported by Tradition and Sciencehaiquy174Încă nu există evaluări
- Catalog Nanoplant PDFDocument26 paginiCatalog Nanoplant PDFAydın AdakÎncă nu există evaluări
- Workshop 0708Document3 paginiWorkshop 0708Manojkumar NairÎncă nu există evaluări
- Aneurysmal Subarachnoid Hemorrhage.6Document19 paginiAneurysmal Subarachnoid Hemorrhage.6Aldy Setiawan PutraÎncă nu există evaluări
- Dry Needling in Lateral Epicondylitis A Prospective EBP PDFDocument5 paginiDry Needling in Lateral Epicondylitis A Prospective EBP PDFDanielle Denice LacabaÎncă nu există evaluări
- Powerpoint Template FinalDocument53 paginiPowerpoint Template Finalapi-265054719Încă nu există evaluări
- Antimicrobial DrugsDocument24 paginiAntimicrobial DrugsMuh Akbar BaharÎncă nu există evaluări
- Eye and Ear Disorders UpdatedDocument78 paginiEye and Ear Disorders Updatedjose arreolaÎncă nu există evaluări
- Philips TUV LampDocument36 paginiPhilips TUV LampHernán Gil ReyÎncă nu există evaluări
- 2 NdresearchpaperDocument5 pagini2 Ndresearchpaperapi-356685046Încă nu există evaluări
- NCP 1Document4 paginiNCP 1Ke EjieÎncă nu există evaluări
- Spasmophilia Comorbidity in Fibromyalgia SyndromeDocument6 paginiSpasmophilia Comorbidity in Fibromyalgia SyndromenovywardanaÎncă nu există evaluări
- Diagnostic Evaluation of Stroke Etiology: Review ArticleDocument13 paginiDiagnostic Evaluation of Stroke Etiology: Review Articleveerraju tvÎncă nu există evaluări
- Sleep Apnea Research PaperDocument9 paginiSleep Apnea Research Paperaflbuagdw100% (3)
- When Death Is Sought - Assisted Suicide and Euthanasia in The Medical ContextDocument5 paginiWhen Death Is Sought - Assisted Suicide and Euthanasia in The Medical ContextMaria Magdalena DumitruÎncă nu există evaluări
- Nomenklatur IBS Edit THTDocument291 paginiNomenklatur IBS Edit THTriezki_pattikratonMDÎncă nu există evaluări
- 2nd Year Speciality MSNDocument5 pagini2nd Year Speciality MSNJennifer DixonÎncă nu există evaluări
- Reflection On Feeding Elderly ClientsDocument2 paginiReflection On Feeding Elderly ClientsLaydee GiaAmÎncă nu există evaluări
- LMA Talk Kelvin 2010 AGDocument26 paginiLMA Talk Kelvin 2010 AGGbotemi AlaladeÎncă nu există evaluări