S-ar putea să vă placă și
- KMC for Neonatal JaundiceDocument65 paginiKMC for Neonatal JaundiceAditi BanerjeeÎncă nu există evaluări
- Assessment of MalingeringDocument12 paginiAssessment of MalingeringkosmicÎncă nu există evaluări
- Medical Devices by FacilityDocument60 paginiMedical Devices by FacilityjwalitÎncă nu există evaluări
- Neonatal JaundiceDocument23 paginiNeonatal Jaundiceamid sultanÎncă nu există evaluări
- Tumor ImmunologyDocument3 paginiTumor ImmunologyStaz Reiya KiraÎncă nu există evaluări
- Neonatal JaundiceDocument33 paginiNeonatal JaundiceVaibhav Krishna100% (2)
- HyperbilirubinemiaDocument49 paginiHyperbilirubinemiaKeith LajotÎncă nu există evaluări
- GPDocument3 paginiGPYwagar YwagarÎncă nu există evaluări
- Approach To Neonatal HyperbilirubinemiaDocument34 paginiApproach To Neonatal HyperbilirubinemiaNilesh HatzadeÎncă nu există evaluări
- Neonatal JaundiceDocument45 paginiNeonatal JaundiceDrhassan HuseinÎncă nu există evaluări
- Neonatal Jaundice and Prolonged Jaundice in Newborn InfantsDocument33 paginiNeonatal Jaundice and Prolonged Jaundice in Newborn InfantskeyRielleÎncă nu există evaluări
- Neonatal Jaundice Cme 3Document56 paginiNeonatal Jaundice Cme 3Arief NorddinÎncă nu există evaluări
- Hyperbilirubinemia: West Visayas State University College of Medicine Neonatal Intensive Care UnitDocument49 paginiHyperbilirubinemia: West Visayas State University College of Medicine Neonatal Intensive Care UnitDonna LabaniegoÎncă nu există evaluări
- Icterus NeonatarumDocument64 paginiIcterus NeonatarumDeepti KukretiÎncă nu există evaluări
- Bilirubin Metabolism: Hd. - Msc. (Biochemistry)Document18 paginiBilirubin Metabolism: Hd. - Msc. (Biochemistry)MuhamadMarufÎncă nu există evaluări
- FINALS TheoreticalDocument6 paginiFINALS TheoreticalCarol Neng Calupitan100% (1)
- Neonatal Jaundice Guide for DoctorsDocument36 paginiNeonatal Jaundice Guide for DoctorsDrMubashir ShaikhÎncă nu există evaluări
- Bilirubin Metabolism GuideDocument41 paginiBilirubin Metabolism GuidefldnazizÎncă nu există evaluări
- Dialogue About A Patient AdmissionDocument3 paginiDialogue About A Patient AdmissionNila Wardana80% (10)
- Kodak Dental 1 Successful Panoramic RadiographyDocument24 paginiKodak Dental 1 Successful Panoramic Radiographymanishbabu100% (2)
- Goal:: Ineffective Airway Clearance Related To Cumulation of SecretionDocument4 paginiGoal:: Ineffective Airway Clearance Related To Cumulation of SecretionWyen CabatbatÎncă nu există evaluări
- Neonatal Jaundice DR - MaslianiDocument58 paginiNeonatal Jaundice DR - MaslianiHengky HanggaraÎncă nu există evaluări
- Neonatal Jaundice Prolonged Jaundice: by Mohd Zamir GhouseDocument18 paginiNeonatal Jaundice Prolonged Jaundice: by Mohd Zamir GhousezamirsgÎncă nu există evaluări
- Approach To Neonatal JaundiceDocument73 paginiApproach To Neonatal JaundiceG Venkatesh50% (2)
- Neonatal Jaundice CmeDocument39 paginiNeonatal Jaundice CmeGideon K. Mutai100% (1)
- Neonatal Jaundice Guide: Causes, Symptoms and TreatmentDocument44 paginiNeonatal Jaundice Guide: Causes, Symptoms and Treatmentmarco luenaÎncă nu există evaluări
- Neonatal Jaundice & HyperbilirubinemiaDocument23 paginiNeonatal Jaundice & HyperbilirubinemiaMeseret Hamer ZewdieÎncă nu există evaluări
- Neonatal Hyperbilirubinemia: Mahlet Abayneh Assistant Professor of PediatricsDocument41 paginiNeonatal Hyperbilirubinemia: Mahlet Abayneh Assistant Professor of PediatricsBegashawÎncă nu există evaluări
- 10 NNJ 1Document22 pagini10 NNJ 1ahmed shorshÎncă nu există evaluări
- Conjugated Bilirubin Direct Bilirubin Unconjugated Bilirubin Indirect BilirubinDocument12 paginiConjugated Bilirubin Direct Bilirubin Unconjugated Bilirubin Indirect BilirubinTanviÎncă nu există evaluări
- Neo JaundiceDocument67 paginiNeo Jaundicemanisha thakur100% (1)
- Paediatric Self ReviewDocument25 paginiPaediatric Self ReviewjyothiÎncă nu există evaluări
- Common Neonatal Problems 2016Document161 paginiCommon Neonatal Problems 2016Dejen TakeleÎncă nu există evaluări
- Neonatal JaundiceDocument11 paginiNeonatal JaundiceImAlien OrGodÎncă nu există evaluări
- Neonatal JaundiceDocument54 paginiNeonatal JaundiceTheresa MendoncaÎncă nu există evaluări
- Care of Neonate With HyperbilirubinemiaDocument11 paginiCare of Neonate With HyperbilirubinemiaKakali ChakrabortyÎncă nu există evaluări
- JAUNDICE ReportDocument33 paginiJAUNDICE ReportMirzi CuisonÎncă nu există evaluări
- Hyper Bilirubin Emi ADocument36 paginiHyper Bilirubin Emi ASai Krishna MaddiralaÎncă nu există evaluări
- Neonatal Jaundice: Bilirubin MetabolismDocument2 paginiNeonatal Jaundice: Bilirubin MetabolismghsÎncă nu există evaluări
- Approach To Neonatal HyperbilirubinemiaDocument34 paginiApproach To Neonatal HyperbilirubinemiaNilesh HatzadeÎncă nu există evaluări
- 2 Jaundice in The NBDocument33 pagini2 Jaundice in The NBCheru DugaseÎncă nu există evaluări
- Neonatal JaundiceDocument95 paginiNeonatal JaundiceChidi MbatuegwuÎncă nu există evaluări
- Physiological and Pathological Jaundice in NewbornsDocument21 paginiPhysiological and Pathological Jaundice in NewbornsTina Ann JohnÎncă nu există evaluări
- Neonatal JaundiceDocument48 paginiNeonatal JaundiceRemy MartinsÎncă nu există evaluări
- BiliDocument63 paginiBiliFu Xiao ShanÎncă nu există evaluări
- 19.neonatal JaundiceDocument42 pagini19.neonatal JaundiceWilhellmuss MaukaÎncă nu există evaluări
- 57-Overview of Approach To HyperbilirubinemiaDocument21 pagini57-Overview of Approach To Hyperbilirubinemiakushraj khandelwalÎncă nu există evaluări
- Icterus Neonatorum: (Neonatal Hyperbilirubinemia)Document30 paginiIcterus Neonatorum: (Neonatal Hyperbilirubinemia)Dian Vera WÎncă nu există evaluări
- Heme Metabolism by DR RoomiDocument24 paginiHeme Metabolism by DR RoomiMudassar Roomi100% (1)
- Sol SeminarDocument15 paginiSol SeminarJimach Bol WieÎncă nu există evaluări
- HyperbilirubinemiaDocument32 paginiHyperbilirubinemiav.stephenson headÎncă nu există evaluări
- IMS: Jaundice: ME218 & ME119Document84 paginiIMS: Jaundice: ME218 & ME119huda zainalÎncă nu există evaluări
- Assignment 3 BilirubbinDocument5 paginiAssignment 3 Bilirubbinhaseeb ShafaatÎncă nu există evaluări
- UNIT HyperbilirubinemiaDocument17 paginiUNIT Hyperbilirubinemiaurmila dewanÎncă nu există evaluări
- Biochemistry of Jaundice Group 2 FinalDocument44 paginiBiochemistry of Jaundice Group 2 FinalShanna SolideoÎncă nu există evaluări
- JaundiceDocument24 paginiJaundiceMena AmerÎncă nu există evaluări
- Neonatal Jaundice 2023Document31 paginiNeonatal Jaundice 2023Demelash SolomonÎncă nu există evaluări
- Neonatal Jaundice: Intensive Care Nursery House Staff ManualDocument3 paginiNeonatal Jaundice: Intensive Care Nursery House Staff ManualLinna SriwaningsiÎncă nu există evaluări
- Bilirubin Metabolism and Hyperbilirubinemia in InfantsDocument31 paginiBilirubin Metabolism and Hyperbilirubinemia in InfantsIzza Ayudia HakimÎncă nu există evaluări
- Jaundice 160318164012Document47 paginiJaundice 160318164012Ritik MishraÎncă nu există evaluări
- Jaundice Classification and DiagnosisDocument46 paginiJaundice Classification and DiagnosisKhadijaÎncă nu există evaluări
- Neonatal Jaundice TreatmentDocument80 paginiNeonatal Jaundice Treatmentgeorgeloto12Încă nu există evaluări
- 01 - GLM - JM - 105 - Product Presentation - FinalDocument68 pagini01 - GLM - JM - 105 - Product Presentation - Finalrahim iqbalÎncă nu există evaluări
- Neonatal Jaundice: Carolyn Joy Mendoza-Capisnon Geraldine Marie SalvoDocument46 paginiNeonatal Jaundice: Carolyn Joy Mendoza-Capisnon Geraldine Marie SalvoCarolyn CapisnonÎncă nu există evaluări
- Bilirubin Metabolism and HyperbilirubinaemiasDocument35 paginiBilirubin Metabolism and HyperbilirubinaemiasEuphrasiaÎncă nu există evaluări
- Approch To Neonatal Jaundice: DR Prinka Peads pg1Document57 paginiApproch To Neonatal Jaundice: DR Prinka Peads pg1DrMubashir ShaikhÎncă nu există evaluări
- Neonatal JaundiceDocument26 paginiNeonatal JaundiceMohd MaghyrehÎncă nu există evaluări
- Gallstones: American College of Gastroenterology Common Gastrointestinal ProblemsDocument2 paginiGallstones: American College of Gastroenterology Common Gastrointestinal ProblemsanonÎncă nu există evaluări
- 4 INT Hana Adiva Praditri 22295 BloodFilmtoDiagnoseMalariaDocument6 pagini4 INT Hana Adiva Praditri 22295 BloodFilmtoDiagnoseMalariaHana AdivaÎncă nu există evaluări
- IMNCI Students Handbook PDFDocument93 paginiIMNCI Students Handbook PDFAamira Qureshi100% (4)
- Literature Review For Specimen Labeling and Blood BankDocument3 paginiLiterature Review For Specimen Labeling and Blood Bankapi-236445988Încă nu există evaluări
- Prevention of Odontogenic Infection - Principles of Management - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Document17 paginiPrevention of Odontogenic Infection - Principles of Management - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Vinnie SinghÎncă nu există evaluări
- How To Apply To CPA's Clinical Specialty ProgramDocument20 paginiHow To Apply To CPA's Clinical Specialty ProgramDr Hafiz Sheraz ArshadÎncă nu există evaluări
- Psychiatry IntroductionDocument26 paginiPsychiatry IntroductionMunir AhmedÎncă nu există evaluări
- SterilizationDocument6 paginiSterilizationasfwegereÎncă nu există evaluări
- My ResumeDocument4 paginiMy ResumeJal-Fem AngelesÎncă nu există evaluări
- Wiley Milbank Memorial FundDocument22 paginiWiley Milbank Memorial FundRob21aÎncă nu există evaluări
- Cases Study in Plasma Cell DyscrasiaDocument87 paginiCases Study in Plasma Cell Dyscrasiadrafq2000Încă nu există evaluări
- Baby Gap: The Surprising Truth About America's Infant-Mortality RateDocument2 paginiBaby Gap: The Surprising Truth About America's Infant-Mortality RateJoseph AltmannÎncă nu există evaluări
- TNM Staging Colorectal CADocument2 paginiTNM Staging Colorectal CAbubbrubb20063998Încă nu există evaluări
- Bionator: The Father of Functional OrthodonticsDocument307 paginiBionator: The Father of Functional OrthodonticsApurava Singh100% (3)
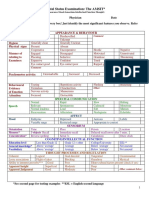
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDocument2 paginiMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- Nurse ResumeDocument1 paginăNurse Resumeapi-400113721Încă nu există evaluări
- Psych 10Document10 paginiPsych 10karenkaren09Încă nu există evaluări
- Meningitis Beyond Neonatal AgeDocument57 paginiMeningitis Beyond Neonatal AgeTilahun Kegne100% (2)
- Academic Style - Practice-1Document5 paginiAcademic Style - Practice-1Anonymous 3s2uAgÎncă nu există evaluări
- SOAP Handout 2010Document4 paginiSOAP Handout 2010wawanÎncă nu există evaluări
- Assessing Body TemperatureDocument6 paginiAssessing Body TemperatureemailÎncă nu există evaluări