S-ar putea să vă placă și
- Tooth Eruption & Shedding MechanismsDocument18 paginiTooth Eruption & Shedding MechanismsAnamika PandeyÎncă nu există evaluări
- Lecture 2 Tooth Eruption and SheddingDocument35 paginiLecture 2 Tooth Eruption and SheddingAMIT GUPTAÎncă nu există evaluări
- Eruption of The TeethDocument15 paginiEruption of The TeethElena CristinaÎncă nu există evaluări
- 1-Eruption of TeethDocument9 pagini1-Eruption of TeethAhmed AbdÎncă nu există evaluări
- CEMENTUMDocument50 paginiCEMENTUMDENTALORG.COM100% (1)
- Dental Anatomy Final ReviewDocument10 paginiDental Anatomy Final ReviewSalma AhmedÎncă nu există evaluări
- Maxillary and Mandibular CanineDocument26 paginiMaxillary and Mandibular CanineShahzeb Memon100% (1)
- Development of Teeth 1Document37 paginiDevelopment of Teeth 1Muli MaroshiÎncă nu există evaluări
- The Periodontium Tissues Supporting TeethDocument78 paginiThe Periodontium Tissues Supporting TeethShuba Prasad100% (1)
- Oral Mucous MembraneDocument200 paginiOral Mucous MembraneKush Pathak100% (3)
- Dentin: QuestionsDocument28 paginiDentin: QuestionssiyaÎncă nu există evaluări
- Periodontal LigamentDocument56 paginiPeriodontal LigamentPurwana Nasir100% (2)
- Atlas of Oral Histology by Akramjuaim PDFDocument151 paginiAtlas of Oral Histology by Akramjuaim PDFAna Maria Hernandez Ardila100% (1)
- CementumDocument18 paginiCementumBahia A RahmanÎncă nu există evaluări
- DentinDocument88 paginiDentinSuhana Ahmed100% (1)
- Word Doc DentinDocument26 paginiWord Doc DentinAditi ChandraÎncă nu există evaluări
- Oral HistologyDocument6 paginiOral HistologyMr. Orange100% (2)
- Space MaintainerDocument36 paginiSpace MaintainerDenis KimÎncă nu există evaluări
- Periodontal LigamentDocument65 paginiPeriodontal LigamentReshmaa Rajendran100% (1)
- Postnatal Craniofacial Skeleton Growth and DevelopmentDocument62 paginiPostnatal Craniofacial Skeleton Growth and DevelopmentDhanusha ReddyÎncă nu există evaluări
- PeriodontiumDocument41 paginiPeriodontiumJay-r Deraya Don100% (1)
- Prenatal and Postnatal Growth of Maxilla and MandibleDocument53 paginiPrenatal and Postnatal Growth of Maxilla and Mandiblekirandeep kaur100% (1)
- Tooth Eruption and Shedding ExplainedDocument29 paginiTooth Eruption and Shedding Explainedjenny girl100% (1)
- Developmental Anomalies of Oral Soft TissuesDocument73 paginiDevelopmental Anomalies of Oral Soft Tissuesvellingiriramesh53040% (1)
- Morphology of Primary Dentition PPT 1Document29 paginiMorphology of Primary Dentition PPT 1Santhoshi ReddyÎncă nu există evaluări
- Alveolar BoneDocument78 paginiAlveolar BoneHarleen GrewalÎncă nu există evaluări
- GicDocument75 paginiGicNihar Arya100% (1)
- Development of Palate and Tongue NotesDocument9 paginiDevelopment of Palate and Tongue NotesClarisse MendozaÎncă nu există evaluări
- Plaque and BiofilmDocument59 paginiPlaque and BiofilmGorremuchu Srinivas100% (2)
- Oral MucosaDocument109 paginiOral Mucosashahzeb memonÎncă nu există evaluări
- Growth & Dev - of MaxillaDocument26 paginiGrowth & Dev - of Maxillaharshita parasharÎncă nu există evaluări
- Seminar Presentation On Enamel: By-Devanshi Sharma P.G.1 Year Dept. of Cons. Dentistry & EndoDocument105 paginiSeminar Presentation On Enamel: By-Devanshi Sharma P.G.1 Year Dept. of Cons. Dentistry & EndoDevanshi SharmaÎncă nu există evaluări
- Dentistry VIVADocument5 paginiDentistry VIVAMatin Ahmad KhanÎncă nu există evaluări
- Anatomy of PalateDocument33 paginiAnatomy of Palatekvellingiri0% (1)
- 2.1 Theories of Dental CariesDocument32 pagini2.1 Theories of Dental CariesCherith M. BañaresÎncă nu există evaluări
- Oral Histology NotesDocument18 paginiOral Histology NotesKhalil Raziq100% (1)
- RPD ImpressionDocument49 paginiRPD ImpressionAmar Bimavarapu0% (1)
- Mandible Development from Prenatal to Postnatal StagesDocument14 paginiMandible Development from Prenatal to Postnatal StagesLiyana G Yaya100% (1)
- 3 - Dentino-Pulp Complex (Mahmoud Bakr)Document129 pagini3 - Dentino-Pulp Complex (Mahmoud Bakr)MobarobberÎncă nu există evaluări
- Growth and Development Maxilla and MandibleDocument42 paginiGrowth and Development Maxilla and MandibleDrMudit Kumar100% (4)
- Enamel: Mineralised Tissue of Ectodermal Origin Covering Anatomic Crowns of Human TeethDocument67 paginiEnamel: Mineralised Tissue of Ectodermal Origin Covering Anatomic Crowns of Human TeethMohammed hisham khan100% (1)
- Muscles of Mastication 2Document80 paginiMuscles of Mastication 2DENTALORG.COMÎncă nu există evaluări
- RPD 2016 Quiz 1 Study GuideDocument9 paginiRPD 2016 Quiz 1 Study Guideapi-296866881Încă nu există evaluări
- DentinDocument76 paginiDentinKhizra Khurram100% (1)
- 1 EnamelDocument40 pagini1 EnamelHarshvardhanÎncă nu există evaluări
- OCCLUSION PPT BY Dr. SumaDocument61 paginiOCCLUSION PPT BY Dr. SumaSuma Tetta100% (2)
- Horizontal Jaw Relation: Centric and Eccentric PositionsDocument37 paginiHorizontal Jaw Relation: Centric and Eccentric Positionsabhijeet100% (1)
- Alveolar Bone: Ist Year ClassDocument47 paginiAlveolar Bone: Ist Year ClassABHINAVÎncă nu există evaluări
- Bleeding Disorders: Presented by Janani RGDocument43 paginiBleeding Disorders: Presented by Janani RGJanani GopalakrishnanÎncă nu există evaluări
- EnamelDocument89 paginiEnamelPavanÎncă nu există evaluări
- 7 - Dentinogenesis PDFDocument14 pagini7 - Dentinogenesis PDFHãnëën Twalbeh83% (12)
- Maxillary Permanent Central IncisorsDocument68 paginiMaxillary Permanent Central IncisorsAmit Singh100% (1)
- Tooth Numbering System Word FileDocument15 paginiTooth Numbering System Word FileRonak PatelÎncă nu există evaluări
- 4-Introduction To Operative Dentistry-1 (1) - 2Document27 pagini4-Introduction To Operative Dentistry-1 (1) - 2MUHAMMAD TAUSEEF SABIRÎncă nu există evaluări
- Introduction To Oral HistologyDocument30 paginiIntroduction To Oral HistologyShalini NairÎncă nu există evaluări
- Oral Histology Questions Part 2Document9 paginiOral Histology Questions Part 2hamzkk100% (3)
- Oral Histology Quiz - What Will Happen If (AmCoFam)Document2 paginiOral Histology Quiz - What Will Happen If (AmCoFam)AmericanCornerFamilyÎncă nu există evaluări
- Oral. H Lec.16Document7 paginiOral. H Lec.16Abdulrahman UdayÎncă nu există evaluări
- 6 - Eruption, Shedding and Maxillary Sinus (Mahmoud Bakr)Document136 pagini6 - Eruption, Shedding and Maxillary Sinus (Mahmoud Bakr)Mobarobber100% (2)
- Lecture 6 Tooth - MovementDocument62 paginiLecture 6 Tooth - MovementThimanthi WithanaÎncă nu există evaluări
- Maxillary SinusDocument31 paginiMaxillary SinusJoachimÎncă nu există evaluări
- Temporomandibular JointDocument78 paginiTemporomandibular JointJoachimÎncă nu există evaluări
- Japanese Anime, Series RecommendationDocument1 paginăJapanese Anime, Series RecommendationJoachimÎncă nu există evaluări
- Chirality: Drawing EnantiomersDocument17 paginiChirality: Drawing EnantiomersJoachimÎncă nu există evaluări
- Alginate Impression Material SettingsDocument2 paginiAlginate Impression Material SettingsJoachimÎncă nu există evaluări
- Experiment 4 - Chemistry 31.1Document7 paginiExperiment 4 - Chemistry 31.1JoachimÎncă nu există evaluări
- Experiment 8B - Chemistry 31.1.Document82 paginiExperiment 8B - Chemistry 31.1.JoachimÎncă nu există evaluări
- Materials For Upper Single Complete Denture ExerciseDocument1 paginăMaterials For Upper Single Complete Denture ExerciseJoachimÎncă nu există evaluări
- STS NotesDocument21 paginiSTS NotesJoachimÎncă nu există evaluări
- Liquid-Liquid Extraction of Benzoic AcidDocument5 paginiLiquid-Liquid Extraction of Benzoic AcidJoachimÎncă nu există evaluări
- Chirality: Drawing EnantiomersDocument17 paginiChirality: Drawing EnantiomersJoachimÎncă nu există evaluări
- Separation of Amino Acids by Paper Chromatography (Rf ValuesDocument4 paginiSeparation of Amino Acids by Paper Chromatography (Rf ValuesJoachimÎncă nu există evaluări
- IsomersDocument28 paginiIsomersPrincess Alyssa AbidÎncă nu există evaluări
- Geometric Isomers: Cis Vs Trans AlkenesDocument10 paginiGeometric Isomers: Cis Vs Trans AlkenesJolaine ValloÎncă nu există evaluări
- Hyman Urogenital SystemDocument3 paginiHyman Urogenital SystemJoachim100% (2)
- Skeleton of The SharkDocument12 paginiSkeleton of The SharkJoachimÎncă nu există evaluări
- 3 Hyman Digestive SystemDocument7 pagini3 Hyman Digestive SystemJoachimÎncă nu există evaluări
- The chicken skeleton: A detailed guideDocument20 paginiThe chicken skeleton: A detailed guideJoachimÎncă nu există evaluări
- Skeleton of The TurtleDocument14 paginiSkeleton of The TurtleJoachim100% (1)
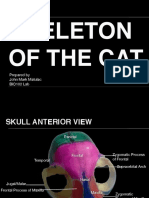
- Skeleton of The Cat: Prepared by John Mark Matulac BIO102 LabDocument27 paginiSkeleton of The Cat: Prepared by John Mark Matulac BIO102 LabJoachimÎncă nu există evaluări
- Why Is Rizal The Greatest Filipino Hero?Document12 paginiWhy Is Rizal The Greatest Filipino Hero?JoachimÎncă nu există evaluări
- Week 1 Day 1Document2 paginiWeek 1 Day 1arens100% (1)
- Argumentative EssayDocument3 paginiArgumentative Essayapi-444150463Încă nu există evaluări
- CHN Assignment (Community Health Nursing)Document21 paginiCHN Assignment (Community Health Nursing)binjuÎncă nu există evaluări
- High Yield Surgery Compatible VersionDocument77 paginiHigh Yield Surgery Compatible Version17kimpÎncă nu există evaluări
- Housing ContractDocument5 paginiHousing Contractapi-225453429100% (1)
- Types of GuidanceDocument13 paginiTypes of GuidanceJomar Gasilla Navarro100% (1)
- What Is Dissociation and What To Do About It?Document2 paginiWhat Is Dissociation and What To Do About It?Tommy ThompsonÎncă nu există evaluări
- General Duties and Responsibilities of An Electrical Engineer in Construction IndustryDocument2 paginiGeneral Duties and Responsibilities of An Electrical Engineer in Construction Industryumer100% (1)
- Cancer Fighting StrategiesDocument167 paginiCancer Fighting StrategiesCaptainjillÎncă nu există evaluări
- K CC1 102 Hse MSDS 005 - R0 EaDocument8 paginiK CC1 102 Hse MSDS 005 - R0 EaWalter Gerardo BelluzÎncă nu există evaluări
- Fundamentals of EU Regulatory Affairs, Fifth Edition Comparative MatrixDocument42 paginiFundamentals of EU Regulatory Affairs, Fifth Edition Comparative Matrixasifmdzakaria57% (7)
- Brosur SucofindoDocument14 paginiBrosur SucofindoJay Van BuurninkÎncă nu există evaluări
- Human Kinetics Library Platform - Benefits and Values of Outdoor RecreationDocument17 paginiHuman Kinetics Library Platform - Benefits and Values of Outdoor RecreationMihail RonnyÎncă nu există evaluări
- Tugas Jurnal TeksolDocument6 paginiTugas Jurnal TeksolNovita IndahÎncă nu există evaluări
- Mds Periodontics Thesis TopicsDocument7 paginiMds Periodontics Thesis Topicsamyholmesmanchester100% (2)
- APSACS Summer Holiday Homework Guide Warm Region 2023 24 Dated 02 June 2023 - CompressedDocument17 paginiAPSACS Summer Holiday Homework Guide Warm Region 2023 24 Dated 02 June 2023 - CompressedGaming 7HawkÎncă nu există evaluări
- Jordan Belliveau DocumentsDocument2 paginiJordan Belliveau DocumentsLeigh Egan100% (1)
- Non-Steroid Analgesic, Antipyretic, Anti-Inflammatory and Anti-Allergy DrugsDocument217 paginiNon-Steroid Analgesic, Antipyretic, Anti-Inflammatory and Anti-Allergy DrugsAstri DesmayantiÎncă nu există evaluări
- Your Body Speaks Your Mind by Deb ShapiroDocument315 paginiYour Body Speaks Your Mind by Deb Shapiroisidora milosevic100% (2)
- Wound HealingDocument44 paginiWound HealingSorin Niky MocanuÎncă nu există evaluări
- NO Kodebarang Satuan Pakai Stock Awal Masuk Keluar Stock Akhir Harga KeteranganDocument4 paginiNO Kodebarang Satuan Pakai Stock Awal Masuk Keluar Stock Akhir Harga Keteranganruang belajar farmasiÎncă nu există evaluări
- Breast Feeding Final ProposalDocument16 paginiBreast Feeding Final ProposalDeborah BoahemaaÎncă nu există evaluări
- Grade 7 (TLE) Week 1Document12 paginiGrade 7 (TLE) Week 1RoswlleÎncă nu există evaluări
- Health Disparities BrochureDocument2 paginiHealth Disparities Brochureapi-276375030100% (1)
- Unit 4 BacteriologyDocument51 paginiUnit 4 BacteriologySharmila LamisharÎncă nu există evaluări
- Admin of Meds Prof GuidanceDocument8 paginiAdmin of Meds Prof GuidanceStacyÎncă nu există evaluări
- Label, Procedure, AdvertisementDocument6 paginiLabel, Procedure, AdvertisementActrissia Aprilla SandhyÎncă nu există evaluări
- Eclampsia Nursing Care Plan - Altered Tissue PerfusionDocument2 paginiEclampsia Nursing Care Plan - Altered Tissue PerfusionCyrus De Asis84% (32)
- Learning Kit - Q3W3 CeslDocument10 paginiLearning Kit - Q3W3 CeslJoselle Batas MagbanuaÎncă nu există evaluări
- Middle Childhood Physical Development (6-11 YearsDocument13 paginiMiddle Childhood Physical Development (6-11 YearsAngela YlaganÎncă nu există evaluări