S-ar putea să vă placă și
- Diabetic Emergencies and ManagementDocument41 paginiDiabetic Emergencies and ManagementNali peterÎncă nu există evaluări
- Acute Complication of DMDocument41 paginiAcute Complication of DMWhite Crime100% (1)
- Assessment - and - Management - of - Patients - With - Diabetes - Mellitus (1) FINALDocument80 paginiAssessment - and - Management - of - Patients - With - Diabetes - Mellitus (1) FINALAMIT MODWALÎncă nu există evaluări
- Diabetic EmergenciesDocument96 paginiDiabetic EmergenciesSoze KeyserÎncă nu există evaluări
- Complications DM FinalDocument57 paginiComplications DM FinalBarbie GirlÎncă nu există evaluări
- Diabetes Mellitus Types 1 & 2: Jessica Perini, MD Sect. Endocrinology WVU Dept of Internal Medicine March 14, 2017Document111 paginiDiabetes Mellitus Types 1 & 2: Jessica Perini, MD Sect. Endocrinology WVU Dept of Internal Medicine March 14, 2017Andres TabaresÎncă nu există evaluări
- Endocrine EmergenciesDocument86 paginiEndocrine Emergenciesadamu mohammadÎncă nu există evaluări
- Diabetes Mellitus 2021Document61 paginiDiabetes Mellitus 2021Andarge ImperialÎncă nu există evaluări
- Case 4 SlidesDocument10 paginiCase 4 SlidesOmar RamadanÎncă nu există evaluări
- Diabetes Younes Ferwana Mohamed MehgizDocument43 paginiDiabetes Younes Ferwana Mohamed MehgizHakim oğluÎncă nu există evaluări
- L11 Diabetes MellitusDocument61 paginiL11 Diabetes MellitusYosra —Încă nu există evaluări
- Lecture - Paediatric Endocrine Emergencies PDFDocument51 paginiLecture - Paediatric Endocrine Emergencies PDFOnSolomonÎncă nu există evaluări
- Deteksi Dini KomplikasiDocument70 paginiDeteksi Dini KomplikasiWiwik Puji LestariÎncă nu există evaluări
- Diabetes Acute Complications - Hypoglycemia and DKADocument37 paginiDiabetes Acute Complications - Hypoglycemia and DKAsilver mistÎncă nu există evaluări
- DIABETIC COMA - Clinical Features and ManagementDocument54 paginiDIABETIC COMA - Clinical Features and ManagementRitesh SinghÎncă nu există evaluări
- ConclusionDocument15 paginiConclusionErlina KusumastutiÎncă nu există evaluări
- Lesson Take-Away - Pathological Conditions Topic One: Diabetes and ComplicationsDocument12 paginiLesson Take-Away - Pathological Conditions Topic One: Diabetes and ComplicationsChantal CarnesÎncă nu există evaluări
- CLP 402: Pharmacotherapy of Diabetes Mellitus: David ShalkurDocument25 paginiCLP 402: Pharmacotherapy of Diabetes Mellitus: David Shalkurbassey etoboÎncă nu există evaluări
- Diabetes MellitusDocument29 paginiDiabetes MellitusIMAFD67% (3)
- DM FinalDocument58 paginiDM FinalMalueth AnguiÎncă nu există evaluări
- Dka (Picucourse)Document33 paginiDka (Picucourse)surasuarezlopezÎncă nu există evaluări
- Diabetes Mellitus: April 2014Document41 paginiDiabetes Mellitus: April 2014Koricho MengistuÎncă nu există evaluări
- KP 5 Endocrine Emergencies 2Document25 paginiKP 5 Endocrine Emergencies 2Fadilla RahmawatiÎncă nu există evaluări
- Endocrine EmergenciesDocument25 paginiEndocrine EmergenciesayaÎncă nu există evaluări
- Acute Care of Diabetes Mellitus: NURS 3071: Acute Health Challenges Feb. 12, 2019Document28 paginiAcute Care of Diabetes Mellitus: NURS 3071: Acute Health Challenges Feb. 12, 2019Savanna ChambersÎncă nu există evaluări
- Paeda DMDocument38 paginiPaeda DMAmanuel LemiÎncă nu există evaluări
- Nephrotic Syndrome in ChildrenDocument33 paginiNephrotic Syndrome in ChildrenAlvin Omondi100% (1)
- Diabetic Ketoacidosis in ChildrenDocument39 paginiDiabetic Ketoacidosis in ChildrenRichard SiahaanÎncă nu există evaluări
- Diabetes MellitusDocument62 paginiDiabetes Mellitusjsmf09Încă nu există evaluări
- Diabetes Mellitus: Prepared by Divya Bhusal B.SC - Nursing 3 YearDocument43 paginiDiabetes Mellitus: Prepared by Divya Bhusal B.SC - Nursing 3 YearSristi LamsalÎncă nu există evaluări
- Diabetes Mellitus: - ClassificationDocument22 paginiDiabetes Mellitus: - ClassificationFernando Junior Parra UchasaraÎncă nu există evaluări
- Med-Lgis-Diabetes Mellitus Complications-Dr. Saima Ambreen Mu1 HFHDocument47 paginiMed-Lgis-Diabetes Mellitus Complications-Dr. Saima Ambreen Mu1 HFHHassan Latif SheikhÎncă nu există evaluări
- Endocrine Emergencies CompiledDocument102 paginiEndocrine Emergencies CompiledSubhkanish RavindraÎncă nu există evaluări
- Askep DMDocument78 paginiAskep DMSiti SangadahÎncă nu există evaluări
- Diabetes MellitusDocument9 paginiDiabetes MellitusM. Joyce100% (2)
- Diabetes Mellitus: Anne Dawnay Biochemical MedicineDocument26 paginiDiabetes Mellitus: Anne Dawnay Biochemical MedicineJoni HermawanÎncă nu există evaluări
- PancreasDocument46 paginiPancreasgzrgythpyjÎncă nu există evaluări
- Diabetes Mellitus DCM 3Document71 paginiDiabetes Mellitus DCM 3maxwell mafungaÎncă nu există evaluări
- TCA Suppression and DM1Document22 paginiTCA Suppression and DM1Rubyrose TagumÎncă nu există evaluări
- Diabetic Emergencies: Sa'ad Lahri Registrar Dept of Emergency MedicineDocument68 paginiDiabetic Emergencies: Sa'ad Lahri Registrar Dept of Emergency MedicineAs ShahirahÎncă nu există evaluări
- Diabetic Emergencies: Sa'ad Lahri Registrar Dept of Emergency MedicineDocument68 paginiDiabetic Emergencies: Sa'ad Lahri Registrar Dept of Emergency MedicineAs ShahirahÎncă nu există evaluări
- Metabolic 1Document81 paginiMetabolic 1Rae SecretariaÎncă nu există evaluări
- Diabetes Care in HospitalizedDocument44 paginiDiabetes Care in HospitalizedArif HandokoÎncă nu există evaluări
- Diabetes Mellitus Type I DMI: Department of Family Medicine and General Practice RcsiDocument25 paginiDiabetes Mellitus Type I DMI: Department of Family Medicine and General Practice RcsikylieverÎncă nu există evaluări
- Diabetes Mellitus Study GuideDocument5 paginiDiabetes Mellitus Study Guiderr5633Încă nu există evaluări
- Pheo Esrd and NeonateDocument45 paginiPheo Esrd and NeonateLea TanÎncă nu există evaluări
- Diabetes Mellitus: NZ Diploma in Enrolled NursingDocument38 paginiDiabetes Mellitus: NZ Diploma in Enrolled NursingRegina PunÎncă nu există evaluări
- Farmakoterapi Sistem Endokrin: Tim Dosen Farmasi KlinikDocument42 paginiFarmakoterapi Sistem Endokrin: Tim Dosen Farmasi KlinikAnonymous h76WT2cFdkÎncă nu există evaluări
- Presenter: Ho. Louis Dor Deng Moderator: DR Pawil Arop Consultant PhysicianDocument60 paginiPresenter: Ho. Louis Dor Deng Moderator: DR Pawil Arop Consultant PhysicianBol Dhalbeny MalualÎncă nu există evaluări
- Adrenal DisordersDocument36 paginiAdrenal DisordersMalueth AnguiÎncă nu există evaluări
- Dka Vs Hhs Edit 1Document25 paginiDka Vs Hhs Edit 1Razeen RiyasatÎncă nu există evaluări
- Perioperative Management 0F Diabetes Mellitus: BY DR - Vamsi Krishna Moderator: DR - RameshDocument46 paginiPerioperative Management 0F Diabetes Mellitus: BY DR - Vamsi Krishna Moderator: DR - Rameshashwini priyaÎncă nu există evaluări
- Endocrinology 3Document56 paginiEndocrinology 3Wonjoo LeeÎncă nu există evaluări
- Diabetic Nephropathy: Yiming Lit, M.D. May 5, 2009Document48 paginiDiabetic Nephropathy: Yiming Lit, M.D. May 5, 2009AraÎncă nu există evaluări
- Acute Complications of Diabetes Mellitus: Hypoglycemia and Hypoglycemic ComaDocument30 paginiAcute Complications of Diabetes Mellitus: Hypoglycemia and Hypoglycemic ComaCristinaGheorgheÎncă nu există evaluări
- Diabetes-Cho 2023 3rd Yr.Document37 paginiDiabetes-Cho 2023 3rd Yr.abdulrahmanbelewa96Încă nu există evaluări
- Diabetic Ketoacidosis: Presented by NG YHDocument32 paginiDiabetic Ketoacidosis: Presented by NG YHYuki NgÎncă nu există evaluări
- Understanding DiabetesDocument83 paginiUnderstanding DiabetesManmeet SÎncă nu există evaluări
- Guidelines For DiabetesDocument43 paginiGuidelines For Diabeteskashiftdr100% (1)
- Hyt Pharma MmeDocument6 paginiHyt Pharma MmeSagnik BhowmikÎncă nu există evaluări
- Physical Examination (Lung)Document14 paginiPhysical Examination (Lung)Huda KamalÎncă nu există evaluări
- Neuroradiology Companion Methods Guidelines and Imaging Fundamentals Zamor PDFDocument1.764 paginiNeuroradiology Companion Methods Guidelines and Imaging Fundamentals Zamor PDFCoralina100% (1)
- Adrian Jess Galindo: DefinitionDocument2 paginiAdrian Jess Galindo: DefinitionAdrian MangahasÎncă nu există evaluări
- 1 Drug Study - DexamethasoneDocument6 pagini1 Drug Study - DexamethasoneJohn100% (1)
- Research On Fasting and Cancer TreatmentDocument9 paginiResearch On Fasting and Cancer TreatmentMÎncă nu există evaluări
- The COC Protocol™ in Pancreatic Cancer - Care Oncology USDocument14 paginiThe COC Protocol™ in Pancreatic Cancer - Care Oncology USStep T.Încă nu există evaluări
- What Is HemiplegiaDocument5 paginiWhat Is HemiplegiaNur AsirahÎncă nu există evaluări
- Kertas Kerja PinjamanDocument18 paginiKertas Kerja PinjamanWan AzmanÎncă nu există evaluări
- Basic Concepts of Pathology and PathophysiologyDocument10 paginiBasic Concepts of Pathology and PathophysiologyIra Agustyne DamanikÎncă nu există evaluări
- 02VBL PemphigusDocument48 pagini02VBL PemphigusRaniya ZainÎncă nu există evaluări
- OHSS Case Presentation Discussion - Jindal IVF CHDDocument41 paginiOHSS Case Presentation Discussion - Jindal IVF CHDJindal IVF ChandigarhÎncă nu există evaluări
- PancretitisDocument44 paginiPancretitisMohammad Husni BanisalmanÎncă nu există evaluări
- Medical Israeli Syllabus For Internal Medicine For Exam LicenseDocument4 paginiMedical Israeli Syllabus For Internal Medicine For Exam Licensemohammadeid0% (2)
- Para PBL CompleteDocument9 paginiPara PBL CompleteMerill Harrelson LibanÎncă nu există evaluări
- Worm Infestations 1Document18 paginiWorm Infestations 1Beta UserÎncă nu există evaluări
- Hydatidiform Mole Study GuideDocument4 paginiHydatidiform Mole Study GuideCarl Elexer Cuyugan AnoÎncă nu există evaluări
- Case Study About Type II Diabetes MellitusDocument82 paginiCase Study About Type II Diabetes MellitusKristine YoungÎncă nu există evaluări
- My Co BacteriumDocument15 paginiMy Co BacteriumPatrickÎncă nu există evaluări
- DashBoard Health SampleDocument1 paginăDashBoard Health SampleAliChana1Încă nu există evaluări
- Formula For Calculating The IV Flow RateDocument16 paginiFormula For Calculating The IV Flow Rateblythe RiveroÎncă nu există evaluări
- Kidney Stones - K.S. GopiDocument4 paginiKidney Stones - K.S. GopiMahmood MuftiÎncă nu există evaluări
- A Patient's Guide To Adhesive CapsulitisDocument6 paginiA Patient's Guide To Adhesive Capsulitisamal sehat100% (1)
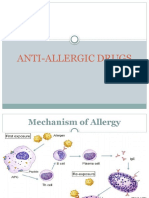
- Anti Allergic DrugsDocument18 paginiAnti Allergic Drugsaamer niaziÎncă nu există evaluări
- Risk Factors Chronic Renal Failure in Rsup ProfDocument8 paginiRisk Factors Chronic Renal Failure in Rsup ProfHanifah Nindy AmaliaÎncă nu există evaluări
- Intravenous ImmunoglobulinDocument6 paginiIntravenous ImmunoglobulinAnastasia TjanÎncă nu există evaluări
- Anesthesia For Trauma Patients 05 Apr 2021 ID40Document10 paginiAnesthesia For Trauma Patients 05 Apr 2021 ID40Erick ToHuÎncă nu există evaluări
- Clinical Fact Sheet PNDocument2 paginiClinical Fact Sheet PNapi-360120287Încă nu există evaluări
- Pain AssessmentDocument33 paginiPain AssessmentmujawayezuÎncă nu există evaluări
- CH 11 IAP Parental Guide On VaccinationDocument9 paginiCH 11 IAP Parental Guide On VaccinationAkankshaKirtiÎncă nu există evaluări