S-ar putea să vă placă și
- 11 BreastDocument22 pagini11 BreastMohammed GhozzÎncă nu există evaluări
- 11 BreastaDocument22 pagini11 BreastaKrishna BalsarzaÎncă nu există evaluări
- Pathology of BreastDocument87 paginiPathology of BreastPandu Harsarapama100% (2)
- Disordered of The Breast: Abdelkarim BarqawiDocument63 paginiDisordered of The Breast: Abdelkarim BarqawiRazan HaimounyÎncă nu există evaluări
- NTU Breast Pathology 2024Document72 paginiNTU Breast Pathology 2024Chen HouyuÎncă nu există evaluări
- Breast Pathology Guide by Dr. Yaniv ZoharDocument109 paginiBreast Pathology Guide by Dr. Yaniv Zoharיוסף יצחק100% (1)
- 3.diseases of The BreastDocument87 pagini3.diseases of The Breastأسود / BlackÎncă nu există evaluări
- Meeting 6 BreastDocument21 paginiMeeting 6 BreastNader KhouryÎncă nu există evaluări
- BreastDocument50 paginiBreastعلي عليÎncă nu există evaluări
- Ovarian TumorsDocument69 paginiOvarian Tumorskarin02Încă nu există evaluări
- female genital pathologyDocument62 paginifemale genital pathologySingitan SiyoumÎncă nu există evaluări
- Common Breast DiseasesDocument64 paginiCommon Breast Diseasesamirahmei100% (1)
- Breast Cancer Presentation FinalDocument69 paginiBreast Cancer Presentation Finalakinpe1100% (1)
- BreastDocument51 paginiBreastmahdi aljamalÎncă nu există evaluări
- Breast Disease and Examination: Dr. Tim CoughlinDocument34 paginiBreast Disease and Examination: Dr. Tim CoughlinDarryl Betts100% (3)
- Breast PathologDocument51 paginiBreast Pathologjusttin779Încă nu există evaluări
- Breast Cancer Risk Factors, Types, Stages, and TreatmentDocument23 paginiBreast Cancer Risk Factors, Types, Stages, and TreatmentArsalan ShaikhÎncă nu există evaluări
- Breast DiseasesDocument35 paginiBreast Diseasesheba1997bshÎncă nu există evaluări
- Breast Cancer Risks, Signs, TreatmentDocument1 paginăBreast Cancer Risks, Signs, TreatmentMelinda Rodriguez RNÎncă nu există evaluări
- Benign Breast Disease111Document55 paginiBenign Breast Disease111Gowtham GanesanÎncă nu există evaluări
- Breast DiseaseDocument17 paginiBreast DiseaseThe Real Uploader100% (1)
- Care of Patients With Cancer of The Cervix and UterusDocument13 paginiCare of Patients With Cancer of The Cervix and UterusJumar ValdezÎncă nu există evaluări
- Cervical Cancer: Santos, Maxime Ella L. Gecera, Alondra KateDocument22 paginiCervical Cancer: Santos, Maxime Ella L. Gecera, Alondra KateLyssaMarieKathryneEgeÎncă nu există evaluări
- Benign Breast Disorders: Diani KartiniDocument27 paginiBenign Breast Disorders: Diani KartiniAngga ArioÎncă nu există evaluări
- Benignbreastdisease DDocument69 paginiBenignbreastdisease DHauwa Shitu JuhaifahÎncă nu există evaluări
- Gynecologic Malignancies: Daniel Breitkopf, MDDocument33 paginiGynecologic Malignancies: Daniel Breitkopf, MDRam Bhupal ReddyÎncă nu există evaluări
- Benign Ovarian TumourDocument45 paginiBenign Ovarian Tumourahmed shorshÎncă nu există evaluări
- Endomaterial Cancer-1Document28 paginiEndomaterial Cancer-1A.H.AÎncă nu există evaluări
- Breast Pathology: Lecturer: Hanina Hibshoosh, M.DDocument35 paginiBreast Pathology: Lecturer: Hanina Hibshoosh, M.DPaulo MartinsÎncă nu există evaluări
- Benign Tumor Malignant Tumor: Ms. Sneha Sehrawat AIIMS RishikeshDocument37 paginiBenign Tumor Malignant Tumor: Ms. Sneha Sehrawat AIIMS RishikeshRajaÎncă nu există evaluări
- Benign Breast DiseasesDocument24 paginiBenign Breast DiseasesNur Hanani KhanÎncă nu există evaluări
- Disease of Female Reproductive System: Maria Picu, MDDocument66 paginiDisease of Female Reproductive System: Maria Picu, MDAbanoub AwadallaÎncă nu există evaluări
- Clinical Features and Investigation of Breast CancerDocument26 paginiClinical Features and Investigation of Breast Cancerጀኔራል አሳምነው ፅጌÎncă nu există evaluări
- BBD-Senior's NoteDocument67 paginiBBD-Senior's NoteK.M.S. ChathunikaÎncă nu există evaluări
- Path Pathology of The Ovaries and Fallopian Tubes Part 1 2020-2021Document12 paginiPath Pathology of The Ovaries and Fallopian Tubes Part 1 2020-2021JohnÎncă nu există evaluări
- Ovarian Tumor Types and TreatmentsDocument36 paginiOvarian Tumor Types and TreatmentsKiran AtlaÎncă nu există evaluări
- Breast Cancer by Professor B. T. UgwuDocument16 paginiBreast Cancer by Professor B. T. UgwuMusaÎncă nu există evaluări
- Uterine (Womb) CancerDocument17 paginiUterine (Womb) Cancerphysio.19bpt1036Încă nu există evaluări
- Xv. Ultrasound Evaluation of The AdnexaDocument13 paginiXv. Ultrasound Evaluation of The AdnexajamiladeguzmanabcdefghijklmÎncă nu există evaluări
- Tumours of The OvaryDocument36 paginiTumours of The OvaryZahidul ZahidÎncă nu există evaluări
- Early Detection of Breast CancerDocument82 paginiEarly Detection of Breast CanceraltamasidartaÎncă nu există evaluări
- Different Pathologies of The UterusDocument74 paginiDifferent Pathologies of The UterusAmal100% (1)
- Benign Breast DisordersDocument30 paginiBenign Breast DisordersShams Nadeem AlamÎncă nu există evaluări
- Approach To An Ovarian Mass - For Students-1Document63 paginiApproach To An Ovarian Mass - For Students-1amq aloqiliÎncă nu există evaluări
- Gestational and Placental Disorders: Obstetric PathologyDocument45 paginiGestational and Placental Disorders: Obstetric PathologyVanessa HermioneÎncă nu există evaluări
- Breast Disorders Assessment GuideDocument26 paginiBreast Disorders Assessment Guideluna nguyenÎncă nu există evaluări
- Breast PresentationDocument45 paginiBreast PresentationEira RajkumarÎncă nu există evaluări
- Benign Disorders and Diseases of The BreastDocument44 paginiBenign Disorders and Diseases of The BreastRoy Acosta GumbanÎncă nu există evaluări
- FGTDocument248 paginiFGTAmanuel MaruÎncă nu există evaluări
- CA Breast New ChangedDocument72 paginiCA Breast New Changedbenak shivalingappaÎncă nu există evaluări
- Endometrial Malignancies 1Document41 paginiEndometrial Malignancies 1jerrydanfordfxÎncă nu există evaluări
- Ovarian TumorDocument59 paginiOvarian Tumorapi-1991639980% (5)
- Non-Neoplastic Disorders of Breast: Dr. Naw May Emerald Faculty of Medicine & Health Sciences UCSI UniversityDocument45 paginiNon-Neoplastic Disorders of Breast: Dr. Naw May Emerald Faculty of Medicine & Health Sciences UCSI UniversitySindhu BabuÎncă nu există evaluări
- Benign Neoplasm of OvaryDocument60 paginiBenign Neoplasm of OvaryMimie SabrinaÎncă nu există evaluări
- Benign Breast Disease EJTLDocument27 paginiBenign Breast Disease EJTLsara01saeedÎncă nu există evaluări
- Carcinoma Endometrium 1Document42 paginiCarcinoma Endometrium 1Sapna SÎncă nu există evaluări
- Carcinomas of The Breast and Genital SystemDocument21 paginiCarcinomas of The Breast and Genital SystemChris QueiklinÎncă nu există evaluări
- Endometrial Cancer: A Comprehensive Resource for Patients and FamiliesDe la EverandEndometrial Cancer: A Comprehensive Resource for Patients and FamiliesÎncă nu există evaluări
- Genital InfectionsDocument50 paginiGenital InfectionsHervis Fantini100% (1)
- Seminar on Alopecia Types and CausesDocument90 paginiSeminar on Alopecia Types and Causesluckyswiss7776848Încă nu există evaluări
- Dealing With Sore ThroatDocument9 paginiDealing With Sore Throatluckyswiss7776848Încă nu există evaluări
- Ob Safe Sex PresentationDocument37 paginiOb Safe Sex Presentationluckyswiss7776848Încă nu există evaluări
- DownloadDocument41 paginiDownloadluckyswiss7776848Încă nu există evaluări
- Cosmetic Surgery Past Present and FutureDocument62 paginiCosmetic Surgery Past Present and Futureluckyswiss7776848Încă nu există evaluări
- Chapter 15bDocument1 paginăChapter 15bluckyswiss7776848Încă nu există evaluări
- Cypt CHT Sti Presentation V1.1enDocument44 paginiCypt CHT Sti Presentation V1.1enluckyswiss7776848Încă nu există evaluări
- Harm Reduction + HIV PresentationDocument110 paginiHarm Reduction + HIV Presentationluckyswiss7776848Încă nu există evaluări
- Campus Sexual Violence FULL VERSIONDocument88 paginiCampus Sexual Violence FULL VERSIONluckyswiss7776848Încă nu există evaluări
- Dance Theory: An Introduction To The FundamentalsDocument69 paginiDance Theory: An Introduction To The Fundamentalsluckyswiss7776848Încă nu există evaluări
- Common Bone Disorders: Bone and Cartilage Deterioration Is A Natural Process As We AgeDocument28 paginiCommon Bone Disorders: Bone and Cartilage Deterioration Is A Natural Process As We Ageluckyswiss7776848Încă nu există evaluări
- Gangrene: by Dr. Nimer Khraim DVMS, BVMS, MVSCDocument18 paginiGangrene: by Dr. Nimer Khraim DVMS, BVMS, MVSCluckyswiss7776848Încă nu există evaluări
- Guidelines For Preoperative Patient Skin AntisepsisDocument49 paginiGuidelines For Preoperative Patient Skin Antisepsisluckyswiss7776848Încă nu există evaluări
- Ch12 Lecture+PPT Kring12eDocument40 paginiCh12 Lecture+PPT Kring12eluckyswiss7776848Încă nu există evaluări
- Lecture 12Document24 paginiLecture 12luckyswiss7776848Încă nu există evaluări
- Testicular CancerDocument48 paginiTesticular Cancerluckyswiss7776848Încă nu există evaluări
- Sexual Disorders ExplainedDocument11 paginiSexual Disorders Explainedluckyswiss7776848Încă nu există evaluări
- Plant DiseasesDocument22 paginiPlant Diseasesluckyswiss7776848Încă nu există evaluări
- Scrotal Masses and Testis TumoursDocument40 paginiScrotal Masses and Testis Tumoursamal.fathullahÎncă nu există evaluări
- Common Bone Disorders: Bone and Cartilage Deterioration Is A Natural Process As We AgeDocument28 paginiCommon Bone Disorders: Bone and Cartilage Deterioration Is A Natural Process As We Ageluckyswiss7776848Încă nu există evaluări
- Common Bone Disorders: Bone and Cartilage Deterioration Is A Natural Process As We AgeDocument28 paginiCommon Bone Disorders: Bone and Cartilage Deterioration Is A Natural Process As We Ageluckyswiss7776848Încă nu există evaluări
- Testicular Tumours Part1Document16 paginiTesticular Tumours Part1luckyswiss7776848Încă nu există evaluări
- 09 Managing Plant DiseasesDocument25 pagini09 Managing Plant Diseasesluckyswiss7776848100% (1)
- Biological Invasions: A Threat To California Ecosystems: - Taught by Dr. Matteo GarbelottoDocument33 paginiBiological Invasions: A Threat To California Ecosystems: - Taught by Dr. Matteo Garbelottoluckyswiss7776848Încă nu există evaluări
- 4 - Plant Disease General ConceptsDocument35 pagini4 - Plant Disease General Conceptsluckyswiss7776848Încă nu există evaluări
- KCP Colon Cancer PowerPoint Feb 2016Document54 paginiKCP Colon Cancer PowerPoint Feb 2016luckyswiss7776848Încă nu există evaluări
- E16 Martial ArtDocument3 paginiE16 Martial Artluckyswiss7776848Încă nu există evaluări
- Ccsc09 12 Att1 CRC Slides Public032009Document27 paginiCcsc09 12 Att1 CRC Slides Public032009luckyswiss7776848Încă nu există evaluări
- Renal Pulmonary EndocrineDocument141 paginiRenal Pulmonary Endocrineluckyswiss7776848Încă nu există evaluări
- Mother's Class BFDocument55 paginiMother's Class BFriz04_fortitudessa5178Încă nu există evaluări
- A Guide For Women With Early Breast Cancer by National Breast Cancer Centre (2003)Document194 paginiA Guide For Women With Early Breast Cancer by National Breast Cancer Centre (2003)john7162Încă nu există evaluări
- Jurnal Tentang Laktasi: Diusulkan OlehDocument10 paginiJurnal Tentang Laktasi: Diusulkan OlehAtun AmbawaniÎncă nu există evaluări
- Mammography: What Is The Goal of Mammography?Document13 paginiMammography: What Is The Goal of Mammography?jeron encaboÎncă nu există evaluări
- Women S Tantric Massage ExperienceDocument12 paginiWomen S Tantric Massage Experiencesicomo0% (2)
- Report Breast FeedingDocument9 paginiReport Breast FeedingMike Faustino SolangonÎncă nu există evaluări
- Design Your Own Anime and Manga Characters - TB ChoiDocument271 paginiDesign Your Own Anime and Manga Characters - TB ChoiEmmanuel Chadee97% (34)
- Mobbs Et Al-2016-Acta PaediatricaDocument7 paginiMobbs Et Al-2016-Acta Paediatricamhelanhie_09Încă nu există evaluări
- Health Education-2Document11 paginiHealth Education-2nishthaÎncă nu există evaluări
- Breast Anatomy and Development GuideDocument8 paginiBreast Anatomy and Development Guidekamie155Încă nu există evaluări
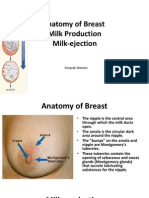
- Anatomy of Breast, Milk Production, and Milk-EjectionDocument23 paginiAnatomy of Breast, Milk Production, and Milk-EjectionDeepak Ghimire100% (2)
- Anatomy of the Female BreastDocument18 paginiAnatomy of the Female Breasthabtsh habshaÎncă nu există evaluări
- Artikel 3Document8 paginiArtikel 3Habibah NursholihahÎncă nu există evaluări
- Essential Guide To Breastfeeding On The Isle of WightDocument28 paginiEssential Guide To Breastfeeding On The Isle of WightMădălinaÎncă nu există evaluări
- Kewirausahaan 10Document118 paginiKewirausahaan 10Rizka Triana FitriÎncă nu există evaluări
- 18 OutgrOwing DeniseDocument62 pagini18 OutgrOwing DeniseVlad Nita50% (4)
- Breast FeedingDocument6 paginiBreast FeedingPradhuymn MishraÎncă nu există evaluări
- Last Requirement OB WardDocument5 paginiLast Requirement OB WardXerxes DejitoÎncă nu există evaluări
- MBFHI Programme of ActivitiesDocument2 paginiMBFHI Programme of ActivitiesEds Asuncion - LapuzÎncă nu există evaluări
- Close Relations An Introduction To The Sociology of Families 6th Edition Mcdaniel Test BankDocument36 paginiClose Relations An Introduction To The Sociology of Families 6th Edition Mcdaniel Test Bankbedwarfratitemmg4100% (26)
- 6066 18318 3 PB (Wadah Penyimpanan)Document6 pagini6066 18318 3 PB (Wadah Penyimpanan)nadyanatasya7Încă nu există evaluări
- Glossary of Radiology Signs by SystemsDocument2 paginiGlossary of Radiology Signs by SystemsIssa OliverÎncă nu există evaluări
- Research Methods Final PaperDocument18 paginiResearch Methods Final Paperapi-449754716Încă nu există evaluări
- An Evening With My Sister-In-lawDocument15 paginiAn Evening With My Sister-In-lawconvenconvenÎncă nu există evaluări
- Examination of The BreastDocument2 paginiExamination of The BreastAufi FillaÎncă nu există evaluări
- Priya and Sripriya - Part 3Document7 paginiPriya and Sripriya - Part 3rishabÎncă nu există evaluări
- GOAL METDocument3 paginiGOAL METAlvincent D. BinwagÎncă nu există evaluări
- Drugs Used in Disorders of Endocrine System Ppt. Book (Lectures 1-6)Document467 paginiDrugs Used in Disorders of Endocrine System Ppt. Book (Lectures 1-6)Marc Imhotep Cray, M.D.Încă nu există evaluări
- Breast ExaminationDocument40 paginiBreast ExaminationSanjay Kumar SanjuÎncă nu există evaluări
- Breast Changes During Pregnancy: Areola Enlarged, Nipple More SensitiveDocument2 paginiBreast Changes During Pregnancy: Areola Enlarged, Nipple More Sensitivenina nikmahÎncă nu există evaluări