S-ar putea să vă placă și
- Management of Organ Failure in Severe MalariaThe provided title "TITLE Management of Organ Failure in Severe MalariaDocument55 paginiManagement of Organ Failure in Severe MalariaThe provided title "TITLE Management of Organ Failure in Severe Malariastivana26Încă nu există evaluări
- Management of Severe Malaria: Paul N HarijantoDocument62 paginiManagement of Severe Malaria: Paul N Harijantostivana26Încă nu există evaluări
- Malaria & HIVDocument17 paginiMalaria & HIVHefie BuahHati MamaAyahÎncă nu există evaluări
- Slide Pathogenesis of Severe MalariaDocument40 paginiSlide Pathogenesis of Severe Malariastivana26Încă nu există evaluări
- Malaria Prevention TimikaDocument41 paginiMalaria Prevention Timikastivana26Încă nu există evaluări
- 1 - Uncomplicated Malaria and TreatmentDocument35 pagini1 - Uncomplicated Malaria and Treatmentstivana26Încă nu există evaluări
- Slide Malaria Prevention TimikaDocument45 paginiSlide Malaria Prevention Timikastivana26Încă nu există evaluări
- Malaria Global Epidemiology Timika Training 20 Nov 2017Document24 paginiMalaria Global Epidemiology Timika Training 20 Nov 2017stivana26Încă nu există evaluări
- Overview of Severe Malaria and Antimalarial For Severe MalariaDocument76 paginiOverview of Severe Malaria and Antimalarial For Severe Malariastivana26Încă nu există evaluări
- Management of Organ Failure in Severe MalariaThe provided title "TITLE Management of Organ Failure in Severe MalariaDocument55 paginiManagement of Organ Failure in Severe MalariaThe provided title "TITLE Management of Organ Failure in Severe Malariastivana26Încă nu există evaluări
- Manifes Mal-Berat Timika-16Document70 paginiManifes Mal-Berat Timika-16stivana26Încă nu există evaluări
- Malaria Global Epidemiology Timika Training 20 Nov 2017Document24 paginiMalaria Global Epidemiology Timika Training 20 Nov 2017stivana26Încă nu există evaluări
- Case Dka MalDocument5 paginiCase Dka Malstivana26Încă nu există evaluări
- 2 Case Study Nov2017 Ver2Document61 pagini2 Case Study Nov2017 Ver2stivana26Încă nu există evaluări
- Case DiscussionDocument60 paginiCase Discussionstivana26Încă nu există evaluări
- Case Dka MalDocument5 paginiCase Dka Malstivana26Încă nu există evaluări
- Malaria & HIVDocument17 paginiMalaria & HIVHefie BuahHati MamaAyahÎncă nu există evaluări
- EDS Case Discussion: Management of Severe Malaria with Liver InvolvementDocument6 paginiEDS Case Discussion: Management of Severe Malaria with Liver Involvementstivana26Încă nu există evaluări
- Case StudiesDocument59 paginiCase Studiesstivana26100% (1)
- Case Dka MalDocument5 paginiCase Dka Malstivana26Încă nu există evaluări
- 2 Case Study Nov2017 Ver2Document61 pagini2 Case Study Nov2017 Ver2stivana26Încă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (72)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Deep Vein Thrombosis: EssentialsDocument7 paginiDeep Vein Thrombosis: EssentialsLuthfia RahmaditaÎncă nu există evaluări
- Pneumatoza IntestinalaDocument32 paginiPneumatoza IntestinalaLupsa LauraÎncă nu există evaluări
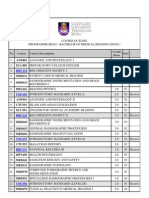
- Course OutlineDocument3 paginiCourse OutlineAmalina JufriÎncă nu există evaluări
- Fumaria OfficinalisDocument9 paginiFumaria OfficinalisPiks DhÎncă nu există evaluări
- Dental Sterilization SOPDocument8 paginiDental Sterilization SOPrahulÎncă nu există evaluări
- Etishree 1999Document7 paginiEtishree 1999Mounik RoutÎncă nu există evaluări
- NCP Imbalanced Nutrition IUGR PatientDocument2 paginiNCP Imbalanced Nutrition IUGR Patientanreilegarde100% (10)
- Balance-Retraining 7Document7 paginiBalance-Retraining 7Pilita Cases NardocciÎncă nu există evaluări
- Systolic Heart FailureDocument66 paginiSystolic Heart FailureFerinaTarizaIIÎncă nu există evaluări
- SOAP Notes Format in EMR: SOAP Stands For Subjective, Objective, Assessment, and PlanDocument2 paginiSOAP Notes Format in EMR: SOAP Stands For Subjective, Objective, Assessment, and PlanNick Jacob100% (7)
- Family Home Remedies by Nadeem Y. MuftiDocument3 paginiFamily Home Remedies by Nadeem Y. MuftinymuftiÎncă nu există evaluări
- TLE Beauty Care Pretest Grade910Document4 paginiTLE Beauty Care Pretest Grade910KENT REEVE ROSALÎncă nu există evaluări
- Antigen Presenting CellsDocument27 paginiAntigen Presenting CellsSajjad AhmadÎncă nu există evaluări
- Pediatrician Power Point 1Document11 paginiPediatrician Power Point 1Ashley100% (1)
- Master's Degree in Periodontology: COURSE 2023-2024Document14 paginiMaster's Degree in Periodontology: COURSE 2023-2024Liseth CarreñoÎncă nu există evaluări
- Terapia Clark Biofeedback ZapperDocument8 paginiTerapia Clark Biofeedback ZapperGomez Gomez50% (2)
- JR Feto NurkulisDocument13 paginiJR Feto NurkulisNurkulis DrÎncă nu există evaluări
- Program Completion Report: School-Based Immunizaton Program (MR-TD HPV)Document3 paginiProgram Completion Report: School-Based Immunizaton Program (MR-TD HPV)Bernivie TenajaÎncă nu există evaluări
- Gynecological Exam GuideDocument2 paginiGynecological Exam GuideLotfyAdelÎncă nu există evaluări
- Yagiela John A Et Al Pharmacology and Therapeutics For Denti1Document1 paginăYagiela John A Et Al Pharmacology and Therapeutics For Denti1AntonPurpurovÎncă nu există evaluări
- ProPublica MethodologyDocument5 paginiProPublica MethodologySouthern California Public RadioÎncă nu există evaluări
- Rabies: Questions and Answers: Information About The Disease and VaccinesDocument4 paginiRabies: Questions and Answers: Information About The Disease and VaccinesgecgecgecÎncă nu există evaluări
- Laparoscopic Hernia SurgeryDocument306 paginiLaparoscopic Hernia SurgeryFrank FpÎncă nu există evaluări
- Independent nurse midwifery practitioner issuesDocument8 paginiIndependent nurse midwifery practitioner issuesKrishnaveni Murugesh100% (3)
- 03TES2011Document999 pagini03TES2011Ahmad IsmatullahÎncă nu există evaluări
- 14 Drug StudyDocument15 pagini14 Drug StudyTricia AlvarezÎncă nu există evaluări
- Makalah KesehatanDocument9 paginiMakalah KesehatanNini RahmiÎncă nu există evaluări
- MGDocument12 paginiMGelektron2010Încă nu există evaluări
- Physiotherapy Roles in Management of Serum BilirubinDocument27 paginiPhysiotherapy Roles in Management of Serum Bilirubinabisinuola8Încă nu există evaluări
- SALIVADocument68 paginiSALIVANimmi RenjithÎncă nu există evaluări