S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Depression in Older Adults: A Treatable Medical ConditionDocument12 paginiDepression in Older Adults: A Treatable Medical ConditionJose Alonso Aguilar Valera100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Unit 7 Bipolar DisorderDocument4 paginiUnit 7 Bipolar DisorderChiriacAioana100% (3)
- Understanding Suicide From Diagnosis To Personalized TreatmentDocument444 paginiUnderstanding Suicide From Diagnosis To Personalized Treatmentbianca_rtjÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Etextbook 978 1305950443 Abnormal Psychology An Integrative ApproachDocument61 paginiEtextbook 978 1305950443 Abnormal Psychology An Integrative Approachmaryann.atkins29094% (48)
- Nelson's MCQ'sDocument150 paginiNelson's MCQ'sDrSheika Bawazir92% (38)
- Postpartum Psychiatric DisordersDocument26 paginiPostpartum Psychiatric DisordersSyakinah SabudinÎncă nu există evaluări
- Mental Status ExaminationDocument8 paginiMental Status ExaminationanisaÎncă nu există evaluări
- IPSRT for Bipolar DisorderDocument16 paginiIPSRT for Bipolar Disorderaastha jain100% (1)
- NCLEX Sample Questions for Psychiatric NursingDocument13 paginiNCLEX Sample Questions for Psychiatric NursingAnaleah MalayaoÎncă nu există evaluări
- Cortex Cerebri (NeoCortex)Document43 paginiCortex Cerebri (NeoCortex)saidahrahmatÎncă nu există evaluări
- SET 2 Oct 27 TRUE KEY ANSWERDocument16 paginiSET 2 Oct 27 TRUE KEY ANSWERJayrald CruzadaÎncă nu există evaluări
- Bipolar Case StudyDocument46 paginiBipolar Case StudyNissie Degulacion100% (1)
- P-Drug FK UmmDocument424 paginiP-Drug FK UmmsaidahrahmatÎncă nu există evaluări
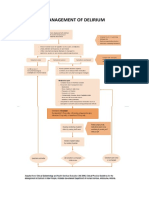
- Management Principles and DeliriumDocument1 paginăManagement Principles and DeliriumsaidahrahmatÎncă nu există evaluări
- Osteoporosis: Fakultas Kedokteran UMM Rumah Sakit Muhammadiyah Lamongan 2017Document2 paginiOsteoporosis: Fakultas Kedokteran UMM Rumah Sakit Muhammadiyah Lamongan 2017saidahrahmatÎncă nu există evaluări
- Skill-Mental and Behavioural Disorders Due To Psychoactive Substance (GMP)Document8 paginiSkill-Mental and Behavioural Disorders Due To Psychoactive Substance (GMP)saidahrahmatÎncă nu există evaluări
- Skill-Paranoid PsychosisDocument7 paginiSkill-Paranoid PsychosissaidahrahmatÎncă nu există evaluări
- Management Principles in Acute PsychosisDocument2 paginiManagement Principles in Acute PsychosissaidahrahmatÎncă nu există evaluări
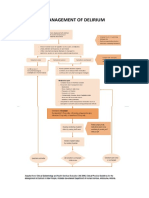
- Management Principles and DeliriumDocument1 paginăManagement Principles and DeliriumsaidahrahmatÎncă nu există evaluări
- Bipolar Disorder Episode DepressionDocument17 paginiBipolar Disorder Episode DepressionfriskaatikaÎncă nu există evaluări
- Skill Hebefrenic SchizophreniaDocument13 paginiSkill Hebefrenic SchizophreniasaidahrahmatÎncă nu există evaluări
- Skill Adjustment DisorderDocument7 paginiSkill Adjustment DisordersaidahrahmatÎncă nu există evaluări
- Skill-Obsessive Compulsive DisorderDocument10 paginiSkill-Obsessive Compulsive DisordersaidahrahmatÎncă nu există evaluări
- Skill-Anxiety7 (Cemas Menyeluruh)Document17 paginiSkill-Anxiety7 (Cemas Menyeluruh)saidahrahmatÎncă nu există evaluări
- Skill Adjustment DisorderDocument7 paginiSkill Adjustment DisordersaidahrahmatÎncă nu există evaluări
- Skill Hebefrenic SchizophreniaDocument13 paginiSkill Hebefrenic SchizophreniasaidahrahmatÎncă nu există evaluări
- Skill Simple SchizophreniaDocument11 paginiSkill Simple SchizophreniasaidahrahmatÎncă nu există evaluări
- Presentation 1Document1 paginăPresentation 1PaulÎncă nu există evaluări
- Paranoid Psychosis: Fadhil Rachma Ferdiana Dessy DwiDocument7 paginiParanoid Psychosis: Fadhil Rachma Ferdiana Dessy DwisaidahrahmatÎncă nu există evaluări
- Management Principles in Acute PsychosisDocument2 paginiManagement Principles in Acute PsychosissaidahrahmatÎncă nu există evaluări
- SOGC Guideline on Diagnosis and Management of EndometriosisDocument36 paginiSOGC Guideline on Diagnosis and Management of EndometriosisreioctabianoÎncă nu există evaluări
- Management Principles and DeliriumDocument1 paginăManagement Principles and DeliriumsaidahrahmatÎncă nu există evaluări
- Skill-Delirium, GGG Psikotik AkutDocument8 paginiSkill-Delirium, GGG Psikotik AkutsaidahrahmatÎncă nu există evaluări
- Immunodeficiency & Autoimmune DisordersDocument20 paginiImmunodeficiency & Autoimmune DisordersZaheer HatsyieÎncă nu există evaluări
- General Biochemistry IIDocument16 paginiGeneral Biochemistry IIsaidahrahmatÎncă nu există evaluări
- Biokimia ObesitasDocument54 paginiBiokimia ObesitassaidahrahmatÎncă nu există evaluări
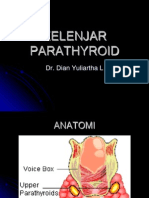
- Kelenjar ParathyroidDocument50 paginiKelenjar ParathyroidsigitdmulyoÎncă nu există evaluări
- Histologi EndokrinDocument23 paginiHistologi EndokrinsaidahrahmatÎncă nu există evaluări
- DeliriumDocument10 paginiDeliriumsaidahrahmatÎncă nu există evaluări
- Petekie, Purpura, EkimosisDocument1 paginăPetekie, Purpura, EkimosissaidahrahmatÎncă nu există evaluări
- Bipolar Disorder and Anxiety Disorder PDFDocument13 paginiBipolar Disorder and Anxiety Disorder PDFLisandrea BrownÎncă nu există evaluări
- WPA Educational Programme On Depressive Disorders PDFDocument98 paginiWPA Educational Programme On Depressive Disorders PDFGe NomÎncă nu există evaluări
- BPCC 133 Guruignou Block-2Document100 paginiBPCC 133 Guruignou Block-2Pulkit HoodaÎncă nu există evaluări
- Psych Questions 1Document34 paginiPsych Questions 1MADHUMITHA VEMULA100% (1)
- Abnormal Psychology ScribblesDocument3 paginiAbnormal Psychology ScribblesNeil Isaac PerezÎncă nu există evaluări
- Instant Download Diagnostic and Statistical Manual of Mental Disorders 5th Edition DSM 5 Ebook PDF PDF ScribdDocument42 paginiInstant Download Diagnostic and Statistical Manual of Mental Disorders 5th Edition DSM 5 Ebook PDF PDF Scribdjeana.gomez838100% (31)
- Kelompok 6 Psi Abnormal ADocument94 paginiKelompok 6 Psi Abnormal Acandle einÎncă nu există evaluări
- Driving Me Crazy - A Representational Analysis of Bipolar Disorder in TelevisionDocument17 paginiDriving Me Crazy - A Representational Analysis of Bipolar Disorder in TelevisionAnnieÎncă nu există evaluări
- Rapid Cycling in Bipolar DisorderDocument1 paginăRapid Cycling in Bipolar Disorderdo leeÎncă nu există evaluări
- Angus Lepp An 2018Document8 paginiAngus Lepp An 2018MadalinaMadaÎncă nu există evaluări
- A Pilot Study of Magnesium Aspartate Droc O de G SI As A Mood Stabilizer For Rapid Cycling Bipolar Affective Disorder PatientsDocument10 paginiA Pilot Study of Magnesium Aspartate Droc O de G SI As A Mood Stabilizer For Rapid Cycling Bipolar Affective Disorder PatientsArhip CojocÎncă nu există evaluări
- Elbaluran Dose Equivelence Drop CardDocument2 paginiElbaluran Dose Equivelence Drop Cardromany hosnyÎncă nu există evaluări
- Materi JNJDocument18 paginiMateri JNJNabila NurfadillaÎncă nu există evaluări
- Literatureand Psychiatryforthe Guardian 222Document11 paginiLiteratureand Psychiatryforthe Guardian 222Oluwafemi GideonÎncă nu există evaluări
- Table 11, DSM-IV To DSM-5 Manic Episode Criteria Comparison - DSM-5 Changes - NCBI BookshelfDocument2 paginiTable 11, DSM-IV To DSM-5 Manic Episode Criteria Comparison - DSM-5 Changes - NCBI BookshelfCÎncă nu există evaluări
- The Bipolar Affective Disorder Dimension Scale (BADDS) - A Dimensional Scale For Rating Lifetime Psychopathology in Bipolar Spectrum DisordersDocument11 paginiThe Bipolar Affective Disorder Dimension Scale (BADDS) - A Dimensional Scale For Rating Lifetime Psychopathology in Bipolar Spectrum DisordersDM YazdaniÎncă nu există evaluări
- Depression GenesDocument12 paginiDepression GenesRayan BotanyÎncă nu există evaluări
- Depression Symptoms and Warning SignsDocument12 paginiDepression Symptoms and Warning SignsVENURI VONARA KUMARASINGHEÎncă nu există evaluări
- Real-Life Clinical Experience With Cariprazine - A Systematic Review of Case StudiesDocument17 paginiReal-Life Clinical Experience With Cariprazine - A Systematic Review of Case Studiesbelloilportogallo99Încă nu există evaluări