S-ar putea să vă placă și
- Pediatric OrthopaedicDocument66 paginiPediatric OrthopaedicDhito RodriguezÎncă nu există evaluări
- Developmental Hip Dysplasia and DislocationDocument51 paginiDevelopmental Hip Dysplasia and Dislocationandi firdha restuwatiÎncă nu există evaluări
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Closed Fractures of The Tibial Diaphysis: David L. Rothberg, MD Erik N. Kubiak, MDDocument64 paginiClosed Fractures of The Tibial Diaphysis: David L. Rothberg, MD Erik N. Kubiak, MDtilahunthmÎncă nu există evaluări
- Hanan Fathy Pediatric Nephrology Unit University of AlexandriaDocument47 paginiHanan Fathy Pediatric Nephrology Unit University of AlexandriadrhananfathyÎncă nu există evaluări
- PSR Talk FinalDocument62 paginiPSR Talk FinalAku Son GraduatesÎncă nu există evaluări
- OsteoarthritisDocument39 paginiOsteoarthritisRohit RajeevÎncă nu există evaluări
- Trauma Spinal Wates Dr. WRDocument68 paginiTrauma Spinal Wates Dr. WRLanlan LesmanaÎncă nu există evaluări
- Fracture FemurDocument21 paginiFracture FemurDanus RamadanusÎncă nu există evaluări
- OSTEOPOROSISDocument33 paginiOSTEOPOROSISSelvaraj ChinnasamyÎncă nu există evaluări
- Management of Trauma PatientDocument18 paginiManagement of Trauma PatientZahir MughalÎncă nu există evaluări
- Bone Tumor Radiology GuideDocument68 paginiBone Tumor Radiology Guideindriyanti natasya ayu utami kottenÎncă nu există evaluări
- Imaging in Maxillofacial TraumaDocument29 paginiImaging in Maxillofacial TraumaAyuAnggayantiÎncă nu există evaluări
- Bone Tumors: Dr. Ahmed HosnyDocument59 paginiBone Tumors: Dr. Ahmed HosnyMohamed MubarkÎncă nu există evaluări
- General Principles of Fracture ManagemenDocument29 paginiGeneral Principles of Fracture ManagemenMichael ThomasÎncă nu există evaluări
- Femur Fxby TahirDocument77 paginiFemur Fxby Tahirtahir mahmood100% (1)
- Introduction To Trauma: LSU Medical Student Clerkship, New Orleans, LADocument31 paginiIntroduction To Trauma: LSU Medical Student Clerkship, New Orleans, LAnandangÎncă nu există evaluări
- Supracondylar FractureDocument53 paginiSupracondylar Fracturedesire kbpÎncă nu există evaluări
- Vascular Diseases: Idar Mappangara Department of Cardiology Hasanuddin UniversityDocument31 paginiVascular Diseases: Idar Mappangara Department of Cardiology Hasanuddin UniversityHariadhii SalamÎncă nu există evaluări
- Musculoskeletal System - Congenital AbnormalitiesDocument49 paginiMusculoskeletal System - Congenital AbnormalitiesShafiq Mohd Nor100% (1)
- Remove clothing, log roll, expose entire body, maintain spinal precautions and warmthDocument29 paginiRemove clothing, log roll, expose entire body, maintain spinal precautions and warmthAjay DherwaniÎncă nu există evaluări
- Ctev NewDocument48 paginiCtev NewDhinie NovianiÎncă nu există evaluări
- Giant Cell TumorDocument22 paginiGiant Cell TumorMaxmillian Alexander KawilarangÎncă nu există evaluări
- Pathological FractureDocument92 paginiPathological FractureSeptyAuliaÎncă nu există evaluări
- Frozen ShoulderDocument29 paginiFrozen ShoulderMárcia PatríciaÎncă nu există evaluări
- Compartment Syndrome: Sebelas Maret UniversityDocument8 paginiCompartment Syndrome: Sebelas Maret Universitykhrisna satyaksaÎncă nu există evaluări
- Reported By: Sr. Jinggle U. Emata John Erick S Enero Calamba Doctors' CollegeDocument35 paginiReported By: Sr. Jinggle U. Emata John Erick S Enero Calamba Doctors' CollegeMarivic DianoÎncă nu există evaluări
- CTEVDocument25 paginiCTEVIceBearÎncă nu există evaluări
- Femoral Shaft FractureDocument44 paginiFemoral Shaft FracturePrabuddha ThihawaÎncă nu există evaluări
- Synovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandSynovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsÎncă nu există evaluări
- Fracture of Radius and Ulna 3Document38 paginiFracture of Radius and Ulna 3Noor Al Zahraa AliÎncă nu există evaluări
- Pelvic FractureDocument31 paginiPelvic Fracturepoe3Încă nu există evaluări
- Septic Arthritis & OsteomyelitisDocument42 paginiSeptic Arthritis & OsteomyelitisCabdi WaliÎncă nu există evaluări
- Damage Control Orthopedic - ASWDocument32 paginiDamage Control Orthopedic - ASWAisyah KhumairahÎncă nu există evaluări
- Avascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDe la EverandAvascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsEvaluare: 4 din 5 stele4/5 (2)
- Developmental Dysplasia of The Hip: Muhammad Rizal, DR., SpotDocument36 paginiDevelopmental Dysplasia of The Hip: Muhammad Rizal, DR., Spotshintadevii100% (1)
- UKA: When Would I Do It?Document35 paginiUKA: When Would I Do It?neareastspineÎncă nu există evaluări
- Orthopedic EmergenciesDocument75 paginiOrthopedic EmergenciesAlex beharuÎncă nu există evaluări
- Exam Technique, HNBreast, Thyroid&AbdomenDocument9 paginiExam Technique, HNBreast, Thyroid&AbdomenInsyirah Hatta100% (1)
- UlcerDocument135 paginiUlcerMahir RathodÎncă nu există evaluări
- Pediatric Hip Dysplasia Case StudyDocument13 paginiPediatric Hip Dysplasia Case Studyapi-349474075Încă nu există evaluări
- Medlung Deformity: D D K SDocument5 paginiMedlung Deformity: D D K SManish MauryaÎncă nu există evaluări
- Arnold-Chiari Malformation ProblemsDocument3 paginiArnold-Chiari Malformation ProblemsBíborkaCsutakÎncă nu există evaluări
- Fractures of The Lower LimbDocument50 paginiFractures of The Lower LimbVishwajit Hegde100% (1)
- Osteomyelitis Metabolic Bone DisordersDocument36 paginiOsteomyelitis Metabolic Bone DisordersVishesh JainÎncă nu există evaluări
- Thyroid NeoplasmDocument11 paginiThyroid NeoplasmPravin KumarÎncă nu există evaluări
- Adult Isthmic SpondylolisthesisDocument21 paginiAdult Isthmic SpondylolisthesisNur RahmawatiÎncă nu există evaluări
- CTEV-Hanum Maftukha ADocument30 paginiCTEV-Hanum Maftukha ADevi Fitri AryaniÎncă nu există evaluări
- 2ndary Malignant Tumor BoneDocument2 pagini2ndary Malignant Tumor Bonetahir_the_great2939Încă nu există evaluări
- Neck of Femur FractureDocument36 paginiNeck of Femur FractureAbdulMushib100% (1)
- Congenital Talipes Equino-VarusDocument48 paginiCongenital Talipes Equino-VarusKojo DuncanÎncă nu există evaluări
- Brachial Plexus InjuryDocument20 paginiBrachial Plexus InjurySuci PramadianiÎncă nu există evaluări
- Normal Pressure HydrocephalusDocument59 paginiNormal Pressure Hydrocephalusrys239Încă nu există evaluări
- Pre Operative Planning For Total Hip ArthroplastyDocument78 paginiPre Operative Planning For Total Hip ArthroplastyJulio EspinozaÎncă nu există evaluări
- Surgery Sheet SchemeDocument51 paginiSurgery Sheet SchemeReem E.MÎncă nu există evaluări
- INGUINAL-SCROTAL SWELLINGS GUIDEDocument23 paginiINGUINAL-SCROTAL SWELLINGS GUIDEAzmyza Azmy100% (1)
- Distal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurDocument76 paginiDistal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurToàn Đặng Phan VĩnhÎncă nu există evaluări
- OSTEOTOMIES AROUND THE HIP FinalDocument51 paginiOSTEOTOMIES AROUND THE HIP FinalWasim R. IssaÎncă nu există evaluări
- Step2 Cs DDX and SymptomsDocument8 paginiStep2 Cs DDX and Symptomswalt65Încă nu există evaluări
- SC - Fracture ZMHDocument51 paginiSC - Fracture ZMHMis StromÎncă nu există evaluări
- Imaging of Blunt Abdominal TraumaDocument13 paginiImaging of Blunt Abdominal Traumadimman001Încă nu există evaluări
- JurnalDocument8 paginiJurnalMuhamad Agung SupriyantoÎncă nu există evaluări
- 2.-Seminario Lancet 2016Document11 pagini2.-Seminario Lancet 2016Tony Gomez Luna LeyvaÎncă nu există evaluări
- Balans Cairan & Elektrolit RSTDocument59 paginiBalans Cairan & Elektrolit RSTMuhamad Agung SupriyantoÎncă nu există evaluări
- Tugas Rehab PascalDocument23 paginiTugas Rehab PascalDenny FirdausÎncă nu există evaluări
- Trauma Wajah: Penanganan Luka Wajah Akibat KecelakaanDocument37 paginiTrauma Wajah: Penanganan Luka Wajah Akibat KecelakaanMuhamad Agung SupriyantoÎncă nu există evaluări
- Odontogram by Muhamad Agung SupriyantoDocument20 paginiOdontogram by Muhamad Agung SupriyantoMuhamad Agung SupriyantoÎncă nu există evaluări
- The Use of Electromagnetic Radiation in Thephysiotherapy - PutowskiDocument6 paginiThe Use of Electromagnetic Radiation in Thephysiotherapy - PutowskiMuhamad Agung SupriyantoÎncă nu există evaluări
- Preoperatif Gravid StrokeDocument19 paginiPreoperatif Gravid StrokeMuhamad Agung SupriyantoÎncă nu există evaluări
- p191 PDFDocument7 paginip191 PDFirsyad120Încă nu există evaluări
- Sepsis & SirsDocument55 paginiSepsis & SirsMuhamad Agung SupriyantoÎncă nu există evaluări
- Ablatio Retina Dr. Yanuar SP.MDocument22 paginiAblatio Retina Dr. Yanuar SP.MMeldianaÎncă nu există evaluări
- Achilles TendonDocument30 paginiAchilles TendonNycoÎncă nu există evaluări
- Trauma Wajah: Penanganan Luka Wajah Akibat KecelakaanDocument37 paginiTrauma Wajah: Penanganan Luka Wajah Akibat KecelakaanMuhamad Agung SupriyantoÎncă nu există evaluări
- Paediatric Orthopaedic Conditions GuideDocument73 paginiPaediatric Orthopaedic Conditions GuideMuhamad Agung SupriyantoÎncă nu există evaluări
- Carpal TunnelDocument39 paginiCarpal TunnelNycoÎncă nu există evaluări
- L09 OTA Open TibiaDocument52 paginiL09 OTA Open TibiaNycoÎncă nu există evaluări
- Clavicle FractureDocument121 paginiClavicle FractureMuhamad Agung SupriyantoÎncă nu există evaluări
- Tarsal TunnelDocument42 paginiTarsal TunnelNycoÎncă nu există evaluări
- Local Anesthetics and Regional TechniquesDocument41 paginiLocal Anesthetics and Regional TechniquesMuhamad Agung SupriyantoÎncă nu există evaluări
- Setting Up Emergency Medical Services for Circulation EmergenciesDocument41 paginiSetting Up Emergency Medical Services for Circulation EmergenciesOliver GiroudÎncă nu există evaluări
- Intro to Anesthesia HistoryDocument21 paginiIntro to Anesthesia HistoryubayyumrÎncă nu există evaluări
- Mod 2a BreathDocument36 paginiMod 2a BreathesterÎncă nu există evaluări
- For More Free Medical Powerpoint Presentations Visit WebsiteDocument24 paginiFor More Free Medical Powerpoint Presentations Visit Websitevanstar7Încă nu există evaluări
- Setting Up Emergency Medical Services for Circulation EmergenciesDocument41 paginiSetting Up Emergency Medical Services for Circulation EmergenciesOliver GiroudÎncă nu există evaluări
- Wms GINA 2017 Main Report Tracked Changes For Archive PDFDocument156 paginiWms GINA 2017 Main Report Tracked Changes For Archive PDFAnnisa MiendaÎncă nu există evaluări
- Mod 3c ChestDocument40 paginiMod 3c ChestInggriht Senny BondangÎncă nu există evaluări
- Setting Up Emergency Medical Service: Intensive Course & WorkshopDocument38 paginiSetting Up Emergency Medical Service: Intensive Course & WorkshopDiajengMaria'benedictaOctavianiOsokPrasetyoÎncă nu există evaluări
- Mod 1a Airway BasicDocument42 paginiMod 1a Airway BasicInggriht Senny BondangÎncă nu există evaluări
- Crochet Triple Stitch CardiganDocument4 paginiCrochet Triple Stitch CardiganAnonymous FXsb2M100% (1)
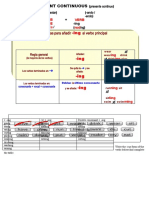
- Reglas para Añadir Al Verbo Principal: Am Is Are ReadDocument8 paginiReglas para Añadir Al Verbo Principal: Am Is Are ReadSamuel Junior Miranda PinzonÎncă nu există evaluări
- Diesel Quick PlayDocument7 paginiDiesel Quick PlaySaúl MolinaÎncă nu există evaluări
- CFT 23Document3 paginiCFT 23Dejan Simonovic PrivatnoÎncă nu există evaluări
- Cheats DB VersionsDocument38 paginiCheats DB VersionsBatalha do CruzeiroÎncă nu există evaluări
- Assignment 6 TextDocument8 paginiAssignment 6 TextPaola AlvaradoÎncă nu există evaluări
- Barbarian Tower Level 20-30 PDFDocument16 paginiBarbarian Tower Level 20-30 PDFIqbal BaihaqiÎncă nu există evaluări
- Chapter 5 RotationDocument24 paginiChapter 5 RotationCHERRY SABASAJEÎncă nu există evaluări
- DK-17 PlanoDocument2 paginiDK-17 PlanoodeiviÎncă nu există evaluări
- BC6900G ManualDocument22 paginiBC6900G ManualMarcela Sava100% (1)
- Ded 4 Semester Exam Aug 2015Document630 paginiDed 4 Semester Exam Aug 2015Iam JaiÎncă nu există evaluări
- Contoh Soal News ItemDocument7 paginiContoh Soal News ItemYehezkiel ImannuelÎncă nu există evaluări
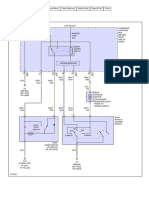
- 2021 Ford Explorer Cell 30 Wire DiagramsDocument35 pagini2021 Ford Explorer Cell 30 Wire Diagramsdarwin perdomoÎncă nu există evaluări
- Chess Score Sheet PDFDocument1 paginăChess Score Sheet PDFRajesh KumarÎncă nu există evaluări
- Trek Volunteer Info Packet 2015Document6 paginiTrek Volunteer Info Packet 2015api-275865446Încă nu există evaluări
- Iyengar Yoga Home Practice Sequences 1 PDFDocument4 paginiIyengar Yoga Home Practice Sequences 1 PDFYogesh Sharma100% (1)
- Chess Pseudonyms PDFDocument31 paginiChess Pseudonyms PDFdon dadaÎncă nu există evaluări
- Baøi Taäp Chöông I: Laäp Moâ Hình ToaùnDocument30 paginiBaøi Taäp Chöông I: Laäp Moâ Hình ToaùnBảo PhươnggÎncă nu există evaluări
- Warfleets FTL - Basic Rulebook v1.8Document15 paginiWarfleets FTL - Basic Rulebook v1.8LucheÎncă nu există evaluări
- Serie ADocument4 paginiSerie AJhon Hernandez RamirezÎncă nu există evaluări
- Toggle Select Wire Mode to Find and Trace Wiring ConnectionsDocument2 paginiToggle Select Wire Mode to Find and Trace Wiring ConnectionsJhon ConnorÎncă nu există evaluări
- Mini Project ReportDocument20 paginiMini Project ReportBhumika MittapelliÎncă nu există evaluări
- War Diary - Sept 1942Document180 paginiWar Diary - Sept 1942Seaforth WebmasterÎncă nu există evaluări
- 11 Lecture PPT Rectilinear MotionDocument42 pagini11 Lecture PPT Rectilinear MotionSim Je Han67% (3)
- Histology LabDocument9 paginiHistology Labsidro123100% (1)
- One Piece Monster Manual - Strong World - GM BinderDocument12 paginiOne Piece Monster Manual - Strong World - GM BinderLuis MartínezÎncă nu există evaluări
- Kit TransmisionDocument45 paginiKit TransmisionJose Carlos Troncoso SarachoÎncă nu există evaluări
- Cali Move - Mobility - Exercise LexiconDocument18 paginiCali Move - Mobility - Exercise LexiconΣτέφανος ΜιχαηλίδηςÎncă nu există evaluări
- Toyota HiluxDocument34 paginiToyota HiluxLeo Te100% (6)
- 3rd IFK U-18 World Tournament WelcomeDocument50 pagini3rd IFK U-18 World Tournament WelcomeBudo MediaÎncă nu există evaluări