S-ar putea să vă placă și
- Apple BenifitsDocument8 paginiApple Benifitsnara4allÎncă nu există evaluări
- Psychotropic DrugsDocument81 paginiPsychotropic DrugsJoan100% (2)
- PREBORD NLE8part1Document671 paginiPREBORD NLE8part1Bryan NorwayneÎncă nu există evaluări
- Postural DeviationsDocument40 paginiPostural DeviationsMohamed Tariq Acchha100% (2)
- Electrolysis, Thermolysis, and The Blend The Principles and Practice of Permanent Hair RemovalDocument328 paginiElectrolysis, Thermolysis, and The Blend The Principles and Practice of Permanent Hair RemovalUmair Ahmad100% (2)
- Pneumonia Management ProtocolDocument2 paginiPneumonia Management Protocolsky nuts100% (1)
- Snakes of South East AsiaDocument24 paginiSnakes of South East AsiaAnonymous HXLczq3Încă nu există evaluări
- Hypertension: Mayur BV BPH 3 Semester PSPHDocument29 paginiHypertension: Mayur BV BPH 3 Semester PSPHBijay Kumar MahatoÎncă nu există evaluări
- 16 Martie - Curs BPOC - SlideDocument95 pagini16 Martie - Curs BPOC - Slidejonah1024Încă nu există evaluări
- Malabsorption: Causes, Symptoms, and TreatmentDocument75 paginiMalabsorption: Causes, Symptoms, and TreatmentLaith Al TamimiÎncă nu există evaluări
- Upper Respiratory Tract InfectionsDocument1 paginăUpper Respiratory Tract Infectionssierranevada123100% (1)
- Management of Pregnancy JaundiceDocument28 paginiManagement of Pregnancy JaundiceShailani Thakur100% (1)
- Hemodiafiltration Kuhlmann PDFDocument31 paginiHemodiafiltration Kuhlmann PDFDavid SantosoÎncă nu există evaluări
- Icu Initial Ventilator SettingsDocument40 paginiIcu Initial Ventilator SettingsantreaspetsasÎncă nu există evaluări
- Clinical Examination of Genitourinary SystemDocument43 paginiClinical Examination of Genitourinary SystemKeamina .aÎncă nu există evaluări
- Group 2 Mrsa 2018aDocument17 paginiGroup 2 Mrsa 2018aDewi PandjukangÎncă nu există evaluări
- Hypertension SPMDocument25 paginiHypertension SPMSai tejendraÎncă nu există evaluări
- Hepatic Failure & Hepatic EncephalopathyDocument37 paginiHepatic Failure & Hepatic Encephalopathyapi-19916399Încă nu există evaluări
- Fulminant Hepatic FailureDocument12 paginiFulminant Hepatic Failureafghansyah arfiantoÎncă nu există evaluări
- Complete Nephrology Revision - c25f1267 7e5b 4cbf b13f 699a5696711aDocument114 paginiComplete Nephrology Revision - c25f1267 7e5b 4cbf b13f 699a5696711aKumarÎncă nu există evaluări
- Neonatus - HIEDocument24 paginiNeonatus - HIEAngeline AdrianneÎncă nu există evaluări
- Acute adrenal insufficiency emergencyDocument6 paginiAcute adrenal insufficiency emergencySteven SetioÎncă nu există evaluări
- Impact of High Sensitivity Troponins For 6nov Cardiac ForumDocument39 paginiImpact of High Sensitivity Troponins For 6nov Cardiac Forummouna6685Încă nu există evaluări
- Pharmacy Budget PreparationDocument15 paginiPharmacy Budget Preparationmamta maliÎncă nu există evaluări
- Cardiac biomarkers: cTnI and NT-proBNPDocument5 paginiCardiac biomarkers: cTnI and NT-proBNPAntonio SessaÎncă nu există evaluări
- Drug Compliance Among Hypertensive PatientsDocument5 paginiDrug Compliance Among Hypertensive PatientsSyifa MunawarahÎncă nu există evaluări
- Liver Cirrhosis PowerPointDocument12 paginiLiver Cirrhosis PowerPointFrancis Adrian100% (2)
- Principles of Nephrology NursingDocument11 paginiPrinciples of Nephrology NursingDhanya RaghuÎncă nu există evaluări
- Rhabdomyolysis: Sheeba Hakak AmnchDocument28 paginiRhabdomyolysis: Sheeba Hakak AmnchMona MorrisÎncă nu există evaluări
- Emergency Medical Condition: Understanding EMTALA RequirementsDocument19 paginiEmergency Medical Condition: Understanding EMTALA RequirementsArlet FlameÎncă nu există evaluări
- Hepatic EncephalopathyDocument21 paginiHepatic EncephalopathyAnonymous n3qy0JdCgÎncă nu există evaluări
- DIABETIC COMA - Clinical Features and ManagementDocument54 paginiDIABETIC COMA - Clinical Features and ManagementRitesh SinghÎncă nu există evaluări
- TB MeningitisDocument17 paginiTB MeningitisSylvan LaminaÎncă nu există evaluări
- Cost EffectivenessDocument22 paginiCost EffectivenessEdalyn CapiliÎncă nu există evaluări
- Corneal UlcersDocument18 paginiCorneal UlcersAvinash NagarÎncă nu există evaluări
- Diagnosi S: MalariaDocument28 paginiDiagnosi S: MalariaOm Prakash SinghÎncă nu există evaluări
- AnthopometryDocument44 paginiAnthopometryghifari2007Încă nu există evaluări
- Esophageal CancerDocument25 paginiEsophageal CancerK poojithaÎncă nu există evaluări
- Treatment of Minor AilmentsDocument43 paginiTreatment of Minor AilmentsVidhya RaniÎncă nu există evaluări
- InhalDocument33 paginiInhallupeÎncă nu există evaluări
- Nephrotic Syndrome: Prepared By: Manisha Praharaj Msc. Nursing 2Nd YearDocument28 paginiNephrotic Syndrome: Prepared By: Manisha Praharaj Msc. Nursing 2Nd YearMaria YaseenÎncă nu există evaluări
- Ectopic PregnancyDocument76 paginiEctopic PregnancyVivian Jean TapayaÎncă nu există evaluări
- Acute Liver Failure: Management of ComplicationsDocument78 paginiAcute Liver Failure: Management of ComplicationsPankaj IngleÎncă nu există evaluări
- 2017 STP Paed Neonates PDFDocument258 pagini2017 STP Paed Neonates PDFChoden JamyangÎncă nu există evaluări
- NHS DIABETESUNDERGOING Surgery Adults Full PDFDocument72 paginiNHS DIABETESUNDERGOING Surgery Adults Full PDFekyÎncă nu există evaluări
- Acute Kidney InjuryDocument21 paginiAcute Kidney InjuryAtif Gazali100% (1)
- Acute Respiratory Failure Concept MapDocument1 paginăAcute Respiratory Failure Concept Mapjenievysenerez100% (1)
- ThalassemiaDocument22 paginiThalassemiaPiyu ShindeÎncă nu există evaluări
- BMT ReportDocument26 paginiBMT ReportCaroline AgbayÎncă nu există evaluări
- National Leprosy Eradication Program (Nlep: Dr. Kanupriya ChaturvediDocument24 paginiNational Leprosy Eradication Program (Nlep: Dr. Kanupriya ChaturvediLavendra KunwarÎncă nu există evaluări
- Hypertensive Emergencies (ESC 2019)Document10 paginiHypertensive Emergencies (ESC 2019)Glen LazarusÎncă nu există evaluări
- Seminar 2 Endocrine DisordersDocument44 paginiSeminar 2 Endocrine DisordersSuganthi ParthibanÎncă nu există evaluări
- Thyroid CrisisDocument11 paginiThyroid CrisisKoka KolaÎncă nu există evaluări
- Pre-Eclampsia, Eclampsia and HELLP SyndromeDocument15 paginiPre-Eclampsia, Eclampsia and HELLP SyndromehendraÎncă nu există evaluări
- Disorders of AortaDocument25 paginiDisorders of Aortavani reddyÎncă nu există evaluări
- HIV Treatment 2Document3 paginiHIV Treatment 2kimglaidyl bontuyanÎncă nu există evaluări
- Case Study About: Cardiac Failure and Pulmonary EdemaDocument32 paginiCase Study About: Cardiac Failure and Pulmonary EdemaIan Simon DorojaÎncă nu există evaluări
- Certificate in Paediatric Nursing: ProgrammeDocument67 paginiCertificate in Paediatric Nursing: ProgrammeWOne WannÎncă nu există evaluări
- GOITERDocument4 paginiGOITERJerika Shane MañosoÎncă nu există evaluări
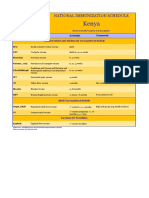
- Kenya Immunization ScheduleDocument1 paginăKenya Immunization ScheduleDani AnyikaÎncă nu există evaluări
- Diabetes Melitus in PregnancyDocument20 paginiDiabetes Melitus in PregnancyAbdulla AlAwadhiÎncă nu există evaluări
- Consumer Protection Act and Patient Bill of RightsDocument17 paginiConsumer Protection Act and Patient Bill of RightsREVATHI H KÎncă nu există evaluări
- RANZCOG CTG Guideline SummaryDocument23 paginiRANZCOG CTG Guideline SummaryAndi Farid AÎncă nu există evaluări
- Hepatic EncephalopathyDocument11 paginiHepatic Encephalopathyjulius billiÎncă nu există evaluări
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesDe la EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesÎncă nu există evaluări
- Dc81b Colour Out of Space Ver 001Document3 paginiDc81b Colour Out of Space Ver 001Victor Guido PinheiroÎncă nu există evaluări
- Definition-Acute Kidney InjuryDocument6 paginiDefinition-Acute Kidney Injuryashi leginÎncă nu există evaluări
- Surgical Abdomen of The Cattle - Descripcion Tecnica Laparotomia Flanco TernerosDocument32 paginiSurgical Abdomen of The Cattle - Descripcion Tecnica Laparotomia Flanco TernerosJhon Bustamante CanoÎncă nu există evaluări
- Traumatic Brain Injury Final 2013.5.29Document59 paginiTraumatic Brain Injury Final 2013.5.29asylum1968Încă nu există evaluări
- Curcuma Longa Extract.: ActionDocument2 paginiCurcuma Longa Extract.: ActionDrShiva PrasadÎncă nu există evaluări
- Aura ArticleDocument6 paginiAura ArticleDharmaMaya ChandrahasÎncă nu există evaluări
- Bioinformatics PaperDocument8 paginiBioinformatics PaperrashigaurÎncă nu există evaluări
- Virulence: Factors in Escherichia Coli Urinary Tract InfectionDocument49 paginiVirulence: Factors in Escherichia Coli Urinary Tract Infectionfajar nugrahaÎncă nu există evaluări
- Revised syllabus for anatomy and physiology coursesDocument40 paginiRevised syllabus for anatomy and physiology coursesSrikutty DevuÎncă nu există evaluări
- Case ReportDocument13 paginiCase Reportfall autumnÎncă nu există evaluări
- Lakshmi V Paed KIMSB 2013Document155 paginiLakshmi V Paed KIMSB 2013Kari RichardsonÎncă nu există evaluări
- Thesis OphthalmologyDocument7 paginiThesis OphthalmologyJames Heller100% (2)
- PPK PTL Copper Silver Ionization Mk2-Ptl Copsil Rev-20110503Document2 paginiPPK PTL Copper Silver Ionization Mk2-Ptl Copsil Rev-20110503Katty TsaiÎncă nu există evaluări
- Obesity Is A Progressive Problem Among Primary School ChildrenDocument15 paginiObesity Is A Progressive Problem Among Primary School ChildrenHimatul MuhimahÎncă nu există evaluări
- Croup: Dr. Shveta Sethi Narula A.P. MicrobiologyDocument14 paginiCroup: Dr. Shveta Sethi Narula A.P. Microbiology12. Akshit AtwalÎncă nu există evaluări
- Stool Analysis GuideDocument28 paginiStool Analysis GuideRajeev PareekÎncă nu există evaluări
- Aditya M Pattewar Et Al 2012Document7 paginiAditya M Pattewar Et Al 2012jsrajoyd_224488661Încă nu există evaluări
- ROJoson PEP Talk: Asymptomatic Gallbladder Polyps Among Seafarers - To Operate or NotDocument36 paginiROJoson PEP Talk: Asymptomatic Gallbladder Polyps Among Seafarers - To Operate or NotrojosonÎncă nu există evaluări
- PDF Dis StandardsDocument35 paginiPDF Dis StandardsEdén PastoraÎncă nu există evaluări
- Valencia - The Rehab Hospital InserviceDocument16 paginiValencia - The Rehab Hospital InserviceVeronica Valencia VictoriaÎncă nu există evaluări
- MSDS Material Safety Data SheetDocument9 paginiMSDS Material Safety Data Sheetpanchoscribd100Încă nu există evaluări
- Comparison Study. CARESCAPEB850Document4 paginiComparison Study. CARESCAPEB850Alberto MHÎncă nu există evaluări
- 12.fixed Partial Denture FailureDocument4 pagini12.fixed Partial Denture FailureArati P HoskhandeÎncă nu există evaluări
- Bioactive and Functional Ingredients From Dairy Products: March 2019Document41 paginiBioactive and Functional Ingredients From Dairy Products: March 2019Fandy RoevÎncă nu există evaluări