S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- 65 FullDocument3 pagini65 FullamereÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Title: A Case of Familial Mediterranean Fever Presented As Renal Amyloidosis Author: Ameer W. Hasan Affiliation: Baghdad Teaching Hospital Case ReportDocument1 paginăTitle: A Case of Familial Mediterranean Fever Presented As Renal Amyloidosis Author: Ameer W. Hasan Affiliation: Baghdad Teaching Hospital Case ReportamereÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- ACR EducationDocument53 paginiACR EducationamereÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Methotrexate and Lung Disease in Rheumatoid ArthritisDocument16 paginiMethotrexate and Lung Disease in Rheumatoid ArthritisamereÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Acetaminophen in Liver DiseaseDocument8 paginiAcetaminophen in Liver DiseaseamereÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Functional Evaluation Magnetic Resonance Imaging: Corelate?Document18 paginiFunctional Evaluation Magnetic Resonance Imaging: Corelate?amereÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Fertility and Pregnancy in Sle 2Document27 paginiFertility and Pregnancy in Sle 2amereÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- DR - Faiq Update Revised 2new BDDocument34 paginiDR - Faiq Update Revised 2new BDamereÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- ACR Case Scenarios 17Document80 paginiACR Case Scenarios 17amereÎncă nu există evaluări
- Lec 2 Seronegative Spondarthritis (Slides)Document66 paginiLec 2 Seronegative Spondarthritis (Slides)amereÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Vaccination Recommendations For Adult Patients With Rheumatic DiseaseDocument21 paginiVaccination Recommendations For Adult Patients With Rheumatic DiseaseamereÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Reactive ArthritisDocument8 paginiReactive ArthritisamereÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Total Joints Rehabilitation-2Document33 paginiTotal Joints Rehabilitation-2amereÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Functional Evaluation Magnetic Resonance Imaging: Corelate ?Document18 paginiFunctional Evaluation Magnetic Resonance Imaging: Corelate ?amereÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Reverensi Kuisioner Oswestry PDFDocument3 paginiReverensi Kuisioner Oswestry PDFagungary95Încă nu există evaluări
- Speech Rehabilitation: Amer WasimDocument28 paginiSpeech Rehabilitation: Amer WasimamereÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- 5.18 ChangDocument16 pagini5.18 Changahmed faroukÎncă nu există evaluări
- Autoantibodies: Prof Sami Salman, FRCP, MRCP, DMR, Ces, MB CHBDocument40 paginiAutoantibodies: Prof Sami Salman, FRCP, MRCP, DMR, Ces, MB CHBamereÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Linezolid Prescribing Guidance November 2013Document5 paginiLinezolid Prescribing Guidance November 2013amereÎncă nu există evaluări
- Annrheumdis 2017 211574.fullDocument8 paginiAnnrheumdis 2017 211574.fullamereÎncă nu există evaluări
- Yasser Seirawan - Winning Chess Brilliancies (Cleaned-Up)Document252 paginiYasser Seirawan - Winning Chess Brilliancies (Cleaned-Up)tudoranluciana183% (12)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- AAGAARD Positional Chess PDFDocument86 paginiAAGAARD Positional Chess PDFAndrew EllanÎncă nu există evaluări
- N N Burdenko Journal of Neurosurgery 2016-06Document108 paginiN N Burdenko Journal of Neurosurgery 2016-06amereÎncă nu există evaluări
- Jadwal Praktek Dokter Spesialis Baru 1akreditasi AllDocument8 paginiJadwal Praktek Dokter Spesialis Baru 1akreditasi Alldonny suryaÎncă nu există evaluări
- Electrical SafetyDocument43 paginiElectrical SafetyVer BautistaÎncă nu există evaluări
- Pediatric Neuropsychology: What Should I Expect?Document2 paginiPediatric Neuropsychology: What Should I Expect?Pradeep JNAÎncă nu există evaluări
- Sex ManualDocument14 paginiSex ManualCally LiueÎncă nu există evaluări
- Emergency Response Drill Scenarios 1Document10 paginiEmergency Response Drill Scenarios 1Arfiyunanto Malika50% (4)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Note Regarding Retiring DoctorsDocument3 paginiNote Regarding Retiring DoctorsnamankumaragrawalÎncă nu există evaluări
- Performance Checklist Enema NOT DoneDocument1 paginăPerformance Checklist Enema NOT DoneMhel MG100% (1)
- Administering MedicationsDocument24 paginiAdministering MedicationsCharmie GandaÎncă nu există evaluări
- Gillentine Alyssa 0362390 11 5 2020Document2 paginiGillentine Alyssa 0362390 11 5 2020api-529380616Încă nu există evaluări
- BooksDocument5 paginiBooksDanijela VukcevicÎncă nu există evaluări
- Resume-Perry Duane GriceDocument4 paginiResume-Perry Duane Griceapi-297972018Încă nu există evaluări
- Alcoholnew 120916093616 Phpapp02 PDFDocument82 paginiAlcoholnew 120916093616 Phpapp02 PDFNihal S KiranÎncă nu există evaluări
- Olympus BF Channels-DesinfDocument1 paginăOlympus BF Channels-DesinfEduardo ArreguinÎncă nu există evaluări
- Aladjem - The Sun Is My Enemy - in Search of The Sun - A Woman's Courageou - Aladjem, Henrietta, 1917 (Orthomolecular Medicine)Document310 paginiAladjem - The Sun Is My Enemy - in Search of The Sun - A Woman's Courageou - Aladjem, Henrietta, 1917 (Orthomolecular Medicine)Anonymous gwFqQcnaX100% (1)
- Detailed Job Description - RaqsDocument3 paginiDetailed Job Description - RaqsBarga John0% (1)
- Pop Q ReferenceDocument18 paginiPop Q ReferenceEdwin KurniawanÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- AOS Injury Classification Systems Poster THORACOLUMBARDocument1 paginăAOS Injury Classification Systems Poster THORACOLUMBARWilliams Maita GallardoÎncă nu există evaluări
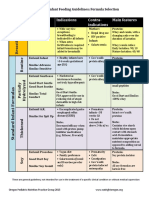
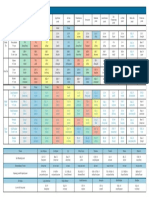
- Formula Selection OPNPGDocument2 paginiFormula Selection OPNPGRina PratiwiÎncă nu există evaluări
- Pulp Therapy in Pediatric DentistryDocument131 paginiPulp Therapy in Pediatric DentistrydrkameshÎncă nu există evaluări
- Supervision ToolsDocument5 paginiSupervision ToolsYaya Taeh Baruh PykÎncă nu există evaluări
- Chapter Review: True or FalseDocument2 paginiChapter Review: True or FalseJames Gabriel SalardaÎncă nu există evaluări
- FD PDFDocument580 paginiFD PDFAinul LuthfiÎncă nu există evaluări
- Bikram Yoga MustDocument5 paginiBikram Yoga Mustratnesh vaviaÎncă nu există evaluări
- Patient AssesmentDocument18 paginiPatient AssesmentMarian Ioan-LucianÎncă nu există evaluări
- Setup Rak ObatDocument161 paginiSetup Rak Obatmuna barajaÎncă nu există evaluări
- Quantum HealingDocument66 paginiQuantum HealingDilek E93% (55)
- Points From Accupuncture AtlasDocument1 paginăPoints From Accupuncture AtlasdishkuÎncă nu există evaluări
- Prenatal DevelopmentDocument29 paginiPrenatal DevelopmentReymart MancaoÎncă nu există evaluări
- List of S-Phrases and R-PhrasesDocument7 paginiList of S-Phrases and R-PhrasesvanyshÎncă nu există evaluări
- Multiple SclerosisDocument96 paginiMultiple SclerosisDrGasnasÎncă nu există evaluări