S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- CTS Flexible Benefit PlanDocument53 paginiCTS Flexible Benefit Plannivasshaan100% (2)
- Lesson 5: Prejudice and StereotypesDocument31 paginiLesson 5: Prejudice and StereotypesZeynep SulaimankulovaÎncă nu există evaluări
- Assignment PSDocument2 paginiAssignment PSMohsin Islam RifatÎncă nu există evaluări
- Presentation On Heavy Engineering Corporation LimitedDocument20 paginiPresentation On Heavy Engineering Corporation LimitedSandeepRajÎncă nu există evaluări
- Allowable Stresses of Typical ASME Materials - Stainless SteelDocument5 paginiAllowable Stresses of Typical ASME Materials - Stainless SteelChanchal K SankaranÎncă nu există evaluări
- Zook Rupture Disc URADocument2 paginiZook Rupture Disc URAmd_taheriÎncă nu există evaluări
- LaserDocument12 paginiLasercabe79Încă nu există evaluări
- English 1 Reading (CVC)Document27 paginiEnglish 1 Reading (CVC)Angelica ArcangelÎncă nu există evaluări
- Excuse Letter1Document1 paginăExcuse Letter1Myiel AngelÎncă nu există evaluări
- Conference Proceedings: Inhaled Nitric Oxide: Delivery Systems and MonitoringDocument27 paginiConference Proceedings: Inhaled Nitric Oxide: Delivery Systems and MonitoringPhanÎncă nu există evaluări
- 432.01 Managing HSE in A Geophysical Nov 2017Document138 pagini432.01 Managing HSE in A Geophysical Nov 2017Andrei Savu100% (1)
- Hello!: I Am Sir DeanDocument30 paginiHello!: I Am Sir DeanDean MalaluanÎncă nu există evaluări
- Afcat Question Paper 01-2014 PDFDocument10 paginiAfcat Question Paper 01-2014 PDFTuhin AzadÎncă nu există evaluări
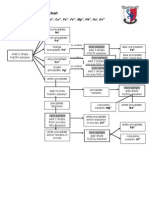
- Testing For Cations Flow ChartDocument2 paginiTesting For Cations Flow Chartapi-252561013Încă nu există evaluări
- Dingenen 2017Document14 paginiDingenen 2017pedro.coleffÎncă nu există evaluări
- Mechanism of Enzyme ActionDocument19 paginiMechanism of Enzyme ActionRubi AnnÎncă nu există evaluări
- 493M GHC MG Mep WS L3 205 1B 00Document1 pagină493M GHC MG Mep WS L3 205 1B 00shehanÎncă nu există evaluări
- GR 15 Juan Esteban Berrio Cordoba Guia 4 ENVIRONMENTAL PROBLEMSDocument7 paginiGR 15 Juan Esteban Berrio Cordoba Guia 4 ENVIRONMENTAL PROBLEMSJuan Esteban Berrio CordobaÎncă nu există evaluări
- Full Download Book Microbiome Immunity Digestive Health and Nutrition Epidemiology Pathophysiology Prevention and Treatment PDFDocument41 paginiFull Download Book Microbiome Immunity Digestive Health and Nutrition Epidemiology Pathophysiology Prevention and Treatment PDFmildred.walker324100% (15)
- Nutrition Label ResponseDocument1 paginăNutrition Label ResponseZoe JonesÎncă nu există evaluări
- Surveys For Maint'Ce ClassDocument7 paginiSurveys For Maint'Ce ClassSuhe EndraÎncă nu există evaluări
- Presentation 2Document70 paginiPresentation 2Vivek LathÎncă nu există evaluări
- VEIKK A15PRO Instruction Manual 0714Document20 paginiVEIKK A15PRO Instruction Manual 0714Corny777 UwUÎncă nu există evaluări
- Vocabulary June v22Document2 paginiVocabulary June v22Wiston TonwisÎncă nu există evaluări
- Exclusively HisDocument129 paginiExclusively HisAngel gargarÎncă nu există evaluări
- VW Golf 8 Variant WD EngDocument664 paginiVW Golf 8 Variant WD EngLakhdar BouchenakÎncă nu există evaluări
- LabStan - July 16-17, 23-24, 30-31, Aug 6-7Document25 paginiLabStan - July 16-17, 23-24, 30-31, Aug 6-7CandypopÎncă nu există evaluări
- Different Types of FermentationDocument26 paginiDifferent Types of FermentationCats and DogÎncă nu există evaluări
- I. External Analysis A. General Environment A. Economic DevelopmentsDocument17 paginiI. External Analysis A. General Environment A. Economic DevelopmentsAndrea TaganginÎncă nu există evaluări
- 1erTareaMicroscopíasLópez Marmolejo Clere MishellDocument4 pagini1erTareaMicroscopíasLópez Marmolejo Clere Mishellclere02marmolejoÎncă nu există evaluări