S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Clinical PresentationsDocument37 paginiClinical PresentationsJim Christian EllaserÎncă nu există evaluări
- Pathophysiology of Peptic Ulcer Disease: Pylori InfectionDocument2 paginiPathophysiology of Peptic Ulcer Disease: Pylori InfectionJim Christian Ellaser100% (1)
- Diagnostic Tests: Community-Acquired PneumoniaDocument23 paginiDiagnostic Tests: Community-Acquired PneumoniaJim Christian EllaserÎncă nu există evaluări
- Pathophysiology PUD 2Document2 paginiPathophysiology PUD 2Jim Christian EllaserÎncă nu există evaluări
- General Objective:: JERIEL Pregnancy-Related BleedingDocument6 paginiGeneral Objective:: JERIEL Pregnancy-Related BleedingJim Christian EllaserÎncă nu există evaluări
- Diagnosis: Congestive Heart Failure Pathophysiology: Differential Diagnosis: Disease/Condition Differentiating Signs/Symptoms Differentiating TestsDocument7 paginiDiagnosis: Congestive Heart Failure Pathophysiology: Differential Diagnosis: Disease/Condition Differentiating Signs/Symptoms Differentiating TestsJim Christian EllaserÎncă nu există evaluări
- SGD #1 Date of Consult: December 5, 2020: Divine Word Hospital Department of Obstetrics and GynecologyDocument1 paginăSGD #1 Date of Consult: December 5, 2020: Divine Word Hospital Department of Obstetrics and GynecologyJim Christian EllaserÎncă nu există evaluări
- Divine Word Hospital Department of Obstetrics and GynecologyDocument1 paginăDivine Word Hospital Department of Obstetrics and GynecologyJim Christian EllaserÎncă nu există evaluări
- SGD #3 Date of Consult: December 11, 2020: Divine Word Hospital Department of Obstetrics and GynecologyDocument2 paginiSGD #3 Date of Consult: December 11, 2020: Divine Word Hospital Department of Obstetrics and GynecologyJim Christian EllaserÎncă nu există evaluări
- SGD #6 Date of Consult: December 19, 2020: Divine Word Hospital Department of Obstetrics and GynecologyDocument3 paginiSGD #6 Date of Consult: December 19, 2020: Divine Word Hospital Department of Obstetrics and GynecologyJim Christian EllaserÎncă nu există evaluări
- Pedia Clinics Sample HX PEDocument6 paginiPedia Clinics Sample HX PEJim Christian EllaserÎncă nu există evaluări
- CaseDocument2 paginiCaseJim Christian EllaserÎncă nu există evaluări
- Divine Word Hospital Department of Obstetrics and GynecologyDocument1 paginăDivine Word Hospital Department of Obstetrics and GynecologyJim Christian EllaserÎncă nu există evaluări
- Typhoid Fever PathophysiologyDocument1 paginăTyphoid Fever PathophysiologyJim Christian EllaserÎncă nu există evaluări
- Algo Acs PDFDocument1 paginăAlgo Acs PDFJim Christian EllaserÎncă nu există evaluări
- Pedia NowDocument9 paginiPedia NowJim Christian EllaserÎncă nu există evaluări
- SURGERY Hemorrhoids PEDocument3 paginiSURGERY Hemorrhoids PEJim Christian EllaserÎncă nu există evaluări
- Hypoxic-Ischemic EncephalopathyDocument34 paginiHypoxic-Ischemic EncephalopathyJim Christian EllaserÎncă nu există evaluări
- Ramel Pedro D. Tadong Post-Graduate Intern Department of PediatricsDocument5 paginiRamel Pedro D. Tadong Post-Graduate Intern Department of PediatricsJim Christian EllaserÎncă nu există evaluări
- Differential Diagnosis: Disease/Condition Differentiating Signs/Symptoms Differentiating TestsDocument3 paginiDifferential Diagnosis: Disease/Condition Differentiating Signs/Symptoms Differentiating TestsJim Christian EllaserÎncă nu există evaluări
- REVISED Pedia Clinics Attendance SheetDocument1 paginăREVISED Pedia Clinics Attendance SheetJim Christian EllaserÎncă nu există evaluări
- Dengue DifferentialsDocument5 paginiDengue DifferentialsJim Christian EllaserÎncă nu există evaluări
- Temperature 38.5C and Claimed To Have 10-20% Weight LossDocument1 paginăTemperature 38.5C and Claimed To Have 10-20% Weight LossJim Christian EllaserÎncă nu există evaluări
- Pathophysiology: Decrease Bile Acid SynthesisDocument1 paginăPathophysiology: Decrease Bile Acid SynthesisJim Christian EllaserÎncă nu există evaluări
- Pedia 2 Year Old M MeningitisDocument8 paginiPedia 2 Year Old M MeningitisJim Christian EllaserÎncă nu există evaluări
- Division of LarynxDocument1 paginăDivision of LarynxJim Christian EllaserÎncă nu există evaluări
- P AncaDocument2 paginiP AncaJim Christian EllaserÎncă nu există evaluări
- Division of LarynxDocument1 paginăDivision of LarynxJim Christian EllaserÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Goals and Learning Objectives of Rotation: Guidelines For LSU Clinical Microbiology RotationDocument4 paginiGoals and Learning Objectives of Rotation: Guidelines For LSU Clinical Microbiology Rotationdrunken monkeyÎncă nu există evaluări
- First Wave of Covid-19 in India and Indonesia-Laptop-Ieskoko7Document37 paginiFirst Wave of Covid-19 in India and Indonesia-Laptop-Ieskoko7Vivek NeelakantanÎncă nu există evaluări
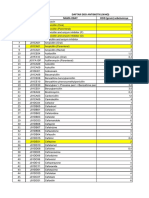
- DAFTAR ATC DDD ANTIBIOTIK WHO 2018 AbcDocument12 paginiDAFTAR ATC DDD ANTIBIOTIK WHO 2018 AbcMahezha DhewaÎncă nu există evaluări
- HIVDocument5 paginiHIVShubham SharmaÎncă nu există evaluări
- GI MnemonicsDocument14 paginiGI Mnemonicsjonnyahn100% (1)
- Parvovirus FinalDocument39 paginiParvovirus FinalJP APÎncă nu există evaluări
- Dengue FeverDocument26 paginiDengue FeverathulpjoseÎncă nu există evaluări
- Presentation, Analysis and Interpretation of FindingsDocument5 paginiPresentation, Analysis and Interpretation of FindingsNgum Jak TongÎncă nu există evaluări
- Mims Abbreviation IndexDocument1 paginăMims Abbreviation IndexHendry RamadhanÎncă nu există evaluări
- Human Papilloma Virus (HPV) : By: Nathalia CruzDocument17 paginiHuman Papilloma Virus (HPV) : By: Nathalia CruzRahmiati LaoÎncă nu există evaluări
- Detailed Micro ChartDocument6 paginiDetailed Micro Chartmatt100% (1)
- BILL GATES KILL On Twitter PDFDocument266 paginiBILL GATES KILL On Twitter PDFCOVID 19 CORONA VIRUS67% (3)
- Q & A Info Sheet PDFDocument3 paginiQ & A Info Sheet PDFJopit Olavario RiveraÎncă nu există evaluări
- Immunization Routine TableDocument9 paginiImmunization Routine TablewenyinriantoÎncă nu există evaluări
- WHO Expert Committee On Biological StandardizationDocument214 paginiWHO Expert Committee On Biological Standardizationcarlosmax5_55Încă nu există evaluări
- Jcuprd1 057181Document11 paginiJcuprd1 057181jhjg9089Încă nu există evaluări
- Elderly Patient History TakingDocument5 paginiElderly Patient History TakinghabbouraÎncă nu există evaluări
- MeningitisDocument15 paginiMeningitisnaveen chaudharyÎncă nu există evaluări
- Separation of Church and StateDocument2 paginiSeparation of Church and StateJann GaliciaÎncă nu există evaluări
- Richland County School District 1 COVID ProtocolsDocument1 paginăRichland County School District 1 COVID ProtocolsWLTXÎncă nu există evaluări
- Thesis HerniaDocument25 paginiThesis HerniaBhageshwar ChaudharyÎncă nu există evaluări
- March, To It Now Being The Vast Majority of Our Sequenced CasesDocument6 paginiMarch, To It Now Being The Vast Majority of Our Sequenced Cases01 LudviaÎncă nu există evaluări
- Amantadine HCLDocument4 paginiAmantadine HCLMae Ann Bueno CastillonÎncă nu există evaluări
- Adult Combined ScheduleDocument6 paginiAdult Combined SchedulesharvaniÎncă nu există evaluări
- APPENDIX 2. Questionnaire Used in The Poultry Industry SurveysDocument38 paginiAPPENDIX 2. Questionnaire Used in The Poultry Industry SurveysAdnan AzamÎncă nu există evaluări
- CVX CodesDocument16 paginiCVX CodesansarÎncă nu există evaluări
- RubellaDocument4 paginiRubellaRose Mary De GuzmanÎncă nu există evaluări
- Awareness and PreventionDocument24 paginiAwareness and Preventionnoname0% (1)
- Antimicrobial Prophylaxis in Oral Surgery and Dental ProceduresDocument9 paginiAntimicrobial Prophylaxis in Oral Surgery and Dental ProceduresMurad AslamÎncă nu există evaluări
- Drug Study - IrinotecanDocument2 paginiDrug Study - IrinotecanTarquin TomadaÎncă nu există evaluări